
Page 211 - Zoo Animal Learning and Training
P. 211
216 Section III: Spinal Procedures
A B
C D
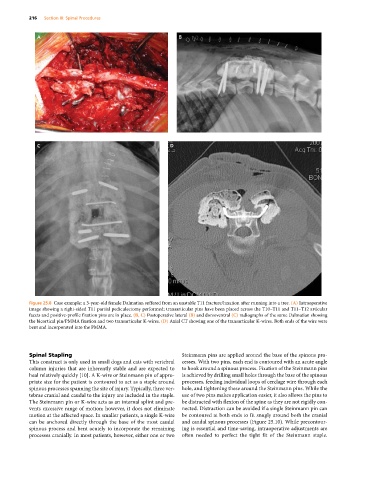
Figure 25.8 Case example: a 3‐year‐old female Dalmatian suffered from an unstable T11 fracture/luxation after running into a tree. (A) Intraoperative
image showing a right‐sided T11 partial pediculectomy performed; transarticular pins have been placed across the T10–T11 and T11–T12 articular
facets and positive‐profile fixation pins are in place. (B, C) Postoperative lateral (B) and dorsoventral (C) radiographs of the same Dalmatian showing
the bicortical pin/PMMA fixation and two transarticular K‐wires. (D) Axial CT showing one of the transarticular K‐wires. Both ends of the wire were
bent and incorporated into the PMMA.
Spinal Stapling Steinmann pins are applied around the base of the spinous pro
This construct is only used in small dogs and cats with vertebral cesses. With two pins, each end is contoured with an acute angle
column injuries that are inherently stable and are expected to to hook around a spinous process. Fixation of the Steinmann pins
heal relatively quickly [10]. A K‐wire or Steinmann pin of appro is achieved by drilling small holes through the base of the spinous
priate size for the patient is contoured to act as a staple around processes, feeding individual loops of cerclage wire through each
spinous processes spanning the site of injury. Typically, three ver hole, and tightening these around the Steinmann pins. While the
tebrae cranial and caudal to the injury are included in the staple. use of two pins makes application easier, it also allows the pins to
The Steinmann pin or K‐wire acts as an internal splint and pre be distracted with flexion of the spine as they are not rigidly con
vents excessive range of motion; however, it does not eliminate nected. Distraction can be avoided if a single Steinmann pin can
motion at the affected space. In smaller patients, a single K‐wire be contoured at both ends to fit snugly around both the cranial
can be anchored directly through the base of the most caudal and caudal spinous processes (Figure 25.10). While precontour
spinous process and bent acutely to incorporate the remaining ing is essential and time‐saving, intraoperative adjustments are
processes cranially. In most patients, however, either one or two often needed to perfect the tight fit of the Steinmann staple.