
Page 686 - Equine Clinical Medicine, Surgery and Reproduction, 2nd Edition
P. 686
Respir atory system: 3.2 Surgical conditions of the respir atory tr act 661
VetBooks.ir tubing it is preferable not to transect an entire tra- 3.108
cheal ring.
Clinical presentation
Mild stenosis may not produce any clinical signs.
Poor performance with harsh respiratory noise is the
typical presentation. A history of prior tracheotomy
surgery is not always available.
Differential diagnosis
Most upper airway obstructions can be included in
the differential diagnosis.
Diagnosis
Diagnosis is by palpation of the trachea and aus-
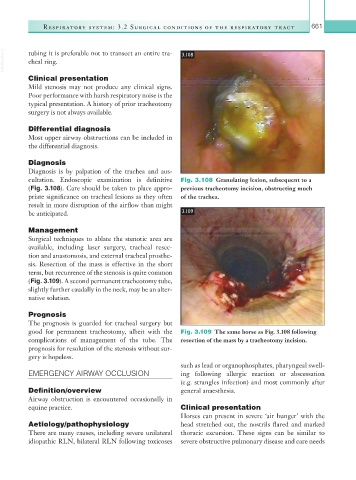
cultation. Endoscopic examination is definitive Fig. 3.108 Granulating lesion, subsequent to a
(Fig. 3.108). Care should be taken to place appro- previous tracheotomy incision, obstructing much
priate significance on tracheal lesions as they often of the trachea.
result in more disruption of the airflow than might
be anticipated. 3.109
Management
Surgical techniques to ablate the stenotic area are
available, including laser surgery, tracheal resec-
tion and anastomosis, and external tracheal prosthe-
sis. Resection of the mass is effective in the short
term, but recurrence of the stenosis is quite common
(Fig. 3.109). A second permanent tracheotomy tube,
slightly further caudally in the neck, may be an alter-
native solution.
Prognosis
The prognosis is guarded for tracheal surgery but
good for permanent tracheotomy, albeit with the Fig. 3.109 The same horse as Fig. 3.108 following
complications of management of the tube. The resection of the mass by a tracheotomy incision.
prognosis for resolution of the stenosis without sur-
gery is hopeless.
such as lead or organophosphates, pharyngeal swell-
EMERGENCY AIRWAY OCCLUSION ing following allergic reaction or abscessation
(e.g. strangles infection) and most commonly after
Definition/overview general anaesthesia.
Airway obstruction is encountered occasionally in
equine practice. Clinical presentation
Horses can present in severe ‘air hunger’ with the
Aetiology/pathophysiology head stretched out, the nostrils flared and marked
There are many causes, including severe unilateral thoracic excursion. These signs can be similar to
idiopathic RLN, bilateral RLN following toxicoses severe obstructive pulmonary disease and care needs