
Page 38 - Small Animal Internal Medicine, 6th Edition
P. 38
10 PART I Cardiovascular System Disorders
midsystole, and then diminishes; the S 1 and S 2 sounds usually Systolic murmurs
can be heard before and after the murmur, respectively. This Systolic murmurs can be decrescendo, holosystolic
VetBooks.ir type is also called an ejection murmur because it occurs (plateau-shaped), or ejection (crescendo-decrescendo) in
configuration. It can be difficult to differentiate these by aus-
during ventricular ejection, usually because of a ventricular
outflow obstruction. A decrescendo murmur tapers from its
diagnosis include establishing that the murmur occurs in
initial intensity over time; it may occur in systole or diastole. cultation alone. However, the most important steps toward
Continuous (machinery) murmurs occur throughout systole systole (rather than diastole), determining its PMI, and
and (well into or) throughout diastole. grading its intensity. Fig. 1.11 depicts the typical PMI of
various murmurs over the chest wall.
Functional, nonpathologic murmurs usually are heard
TABLE 1.1 best over the left heart base. They are soft to moderate in
intensity and of decrescendo or crescendo-decrescendo
Grading of Heart Murmurs configuration. Functional murmurs have no apparent
CV structural cause and can accompany physiologic
GRADE MURMUR
1 Very soft murmur; heard only over its site of
origin, after prolonged listening in quiet
surroundings
2 Soft murmur but easily heard over its site of
origin (usually a particular valve area)
3 Moderate-intensity murmur; usually radiates Holosystolic
to other precordial/valve areas too (plateau, regurgitant)
4 Loud murmur but without a precordial thrill; Crescendo-decrescendo
radiates widely and usually can be heard (diamond-shaped, ejection)
over most precordial regions Systolic decrescendo
5 Loud murmur with a palpable precordial
thrill; radiates widely and usually can be Diastolic decrescendo
heard clearly over all precordial regions
6 Very loud murmur with a precordial thrill; Continuous
radiates widely, generally is heard (machinery)
clearly over all precordial areas, and S 1 S 2 S 1 S 2
also can be heard with the stethoscope
chestpiece lifted slightly (~1 cm) from the FIG 1.10
chest wall (at the murmur PMI) The phonocardiographic shape (configuration) and the
timing of different murmurs are illustrated in this diagram.
A B
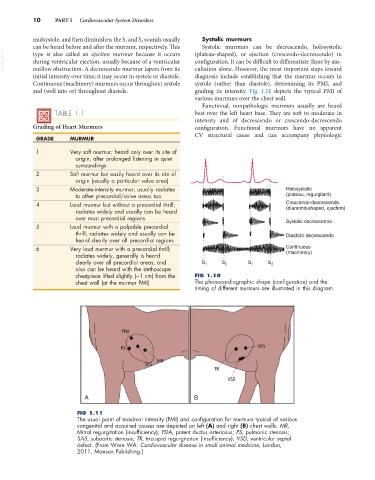
FIG 1.11
The usual point of maximal intensity (PMI) and configuration for murmurs typical of various
congenital and acquired causes are depicted on left (A) and right (B) chest walls. MR,
Mitral regurgitation (insufficiency); PDA, patent ductus arteriosus; PS, pulmonic stenosis;
SAS, subaortic stenosis; TR, tricuspid regurgitation (insufficiency); VSD, ventricular septal
defect. (From Ware WA: Cardiovascular disease in small animal medicine, London,
2011, Manson Publishing.)