
Page 748 - Adams and Stashak's Lameness in Horses, 7th Edition
P. 748
714 Chapter 5
VetBooks.ir
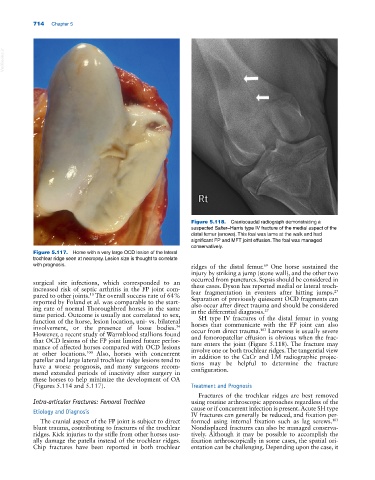
Figure 5.118. Craniocaudal radiograph demonstrating a
suspected Salter–Harris type IV fracture of the medial aspect of the
distal femur (arrows). This foal was lame at the walk and had
significant FP and MFT joint effusion. The foal was managed
conservatively.
Figure 5.117. Horse with a very large OCD lesion of the lateral
trochlear ridge seen at necropsy. Lesion size is thought to correlate
with prognosis. ridges of the distal femur. One horse sustained the
69
injury by striking a jump (stone wall), and the other two
occurred from punctures. Sepsis should be considered in
surgical site infections, which corresponded to an these cases. Dyson has reported medial or lateral troch-
increased risk of septic arthritis in the FP joint com- lear fragmentation in eventers after hitting jumps.
27
pared to other joints. The overall success rate of 64% Separation of previously quiescent OCD fragments can
13
reported by Foland et al. was comparable to the start- also occur after direct trauma and should be considered
ing rate of normal Thoroughbred horses in the same in the differential diagnosis. 27
time period. Outcome is usually not correlated to sex, SH type IV fractures of the distal femur in young
function of the horse, lesion location, uni‐ vs. bilateral horses that communicate with the FP joint can also
involvement, or the presence of loose bodies. occur from direct trauma. Lameness is usually severe
34
103
However, a recent study of Warmblood stallions found and femoropatellar effusion is obvious when the frac-
that OCD lesions of the FP joint limited future perfor- ture enters the joint (Figure 5.118). The fracture may
mance of affected horses compared with OCD lesions involve one or both trochlear ridges. The tangential view
at other locations. Also, horses with concurrent in addition to the CaCr and LM radiographic projec-
100
patellar and large lateral trochlear ridge lesions tend to tions may be helpful to determine the fracture
have a worse prognosis, and many surgeons recom- configuration.
mend extended periods of inactivity after surgery in
these horses to help minimize the development of OA
(Figures 5.114 and 5.117). Treatment and Prognosis
Fractures of the trochlear ridges are best removed
Intra‐articular Fractures: Femoral Trochlea using routine arthroscopic approaches regardless of the
cause or if concurrent infection is present. Acute SH type
Etiology and Diagnosis
IV fractures can generally be reduced, and fixation per-
The cranial aspect of the FP joint is subject to direct formed using internal fixation such as lag screws.
103
blunt trauma, contributing to fractures of the trochlear Nondisplaced fractures can also be managed conserva-
ridges. Kick injuries to the stifle from other horses usu- tively. Although it may be possible to accomplish the
ally damage the patella instead of the trochlear ridges. fixation arthroscopically in some cases, the spatial ori-
Chip fractures have been reported in both trochlear entation can be challenging. Depending upon the case, it