
Page 235 - Clinical Small Animal Internal Medicine
P. 235
20 Ventricular Arrhythmias 203
VetBooks.ir
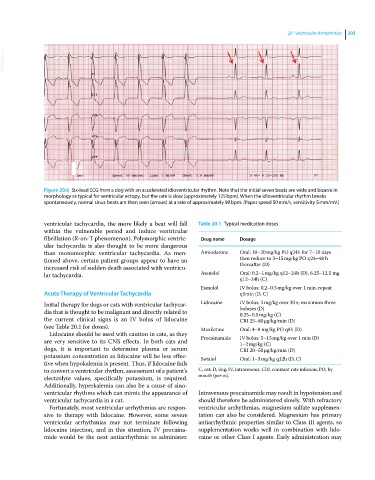
Figure 20.6 Six‐lead ECG from a dog with an accelerated idioventricular rhythm. Note that the initial seven beats are wide and bizarre in
morphology as typical for ventricular ectopy, but the rate is slow (approximately 125 bpm). When the idioventricular rhythm breaks
spontaneously, normal sinus beats are then seen (arrows) at a rate of approximately 90 bpm. (Paper speed 50 mm/s, sensitivity 5 mm/mV.)
ventricular tachycardia, the more likely a beat will fall Table 20.1 Typical medication doses
within the vulnerable period and induce ventricular
fibrillation (R‐on‐T phenomenon). Polymorphic ventric- Drug name Dosage
ular tachycardia is also thought to be more dangerous
than monomorphic ventricular tachycardia. As men- Amiodarone Oral: 10–20 mg/kg PO q24h for 7–10 days
tioned above, certain patient groups appear to have an then reduce to 3–15 mg/kg PO q24–48 h
increased risk of sudden death associated with ventricu- thereafter (D)
lar tachycardia. Atenolol Oral: 0.2–1 mg/kg q12–24h (D), 6.25–12.5 mg
q12–24h (C)
Esmolol IV bolus: 0.2–0.5 mg/kg over 1 min, repeat
Acute Therapy of Ventricular Tachycardia q5min (D, C)
Initial therapy for dogs or cats with ventricular tachycar- Lidocaine IV bolus: 2 mg/kg over 30 s; maximum three
dia that is thought to be malignant and directly related to boluses (D)
0.25–0.5 mg/kg (C)
the current clinical signs is an IV bolus of lidocaine CRI 25–80 μg/kg/min (D)
(see Table 20.1 for doses). Mexiletine Oral: 4–8 mg/kg PO q8h (D)
Lidocaine should be used with caution in cats, as they
are very sensitive to its CNS effects. In both cats and Procainamide IV bolus: 5–15 mg/kg over 1 min (D)
1–2 mg/kg (C)
dogs, it is important to determine plasma or serum CRI 20–50 μg/kg/min (D)
potassium concentration as lidocaine will be less effec- Sotalol Oral: 1–3 mg/kg q12h (D, C)
tive when hypokalemia is present. Thus, if lidocaine fails
to convert a ventricular rhythm, assessment of a patient’s C, cat; D, dog; IV, intravenous; CRI, constant rate infusion; PO, by
electrolyte values, specifically potassium, is required. mouth (per os).
Additionally, hyperkalemia can also be a cause of sino-
ventricular rhythms which can mimic the appearance of Intravenous procainamide may result in hypotension and
ventricular tachycardia in a cat. should therefore be administered slowly. With refractory
Fortunately, most ventricular arrhythmias are respon- ventricular arrhythmias, magnesium sulfate supplemen-
sive to therapy with lidocaine. However, some severe tation can also be considered. Magnesium has primary
ventricular arrhythmias may not terminate following antiarrhythmic properties similar to Class III agents, so
lidocaine injection, and in this situation, IV procaina- supplementation works well in combination with lido-
mide would be the next antiarrhythmic to administer. caine or other Class I agents. Early administration may