
Page 9 - GP Fall 2022_Neat
P. 9
blisters. The ulcerative stage presents with gers of sunlight, stress, fevers and cold are Clinical: An ulcer, by definition, is a break
small superficial discreet ulcers involving the ones most often cited. Herpes labialis is in the epithelium exposing peripheral nerve
only the epithelium that may coalesce to extremely contagious with approximately endings in the lamina propria. There is typi-
form a much larger ulcer. It never involves 85% of the adult population being seropos- cally damage to both the epithelium and the
the connective tissue and does not present itive for antibodies to the virus. Recurrent connective tissue. Each type of ulcer will
with a red halo. For recurrent intraoral her- herpes labialis is a complex problem with present with a slightly different clinical
petic lesions and herpes labialis, the first pronounced psychosocial ramifications, presentation depending upon etiology.
three clinical stages (prodromal, vesicular, most notably the clinical morbidities of
and ulcerative) are the same. Scabbing does pain, possible transmission of the virus to Etiology: There is no known etiology.
not occur in a wet environment, therefore others, and social embarrassment.
intraoral lesions do not form a crust but Clinical: Recurrent minor aphthous ul-
heal from the bottom up and periphery in. Treatment: Current care has centered on cers or recurrent aphthous stomatitis are
Herpes labialis develops only on the ver- both topical and systemic antiviral thera- commonly known by the general popula-
million border of the lip and is considered pies. These antiviral medications interrupt tion as canker sores. They are clearly de-
to be of skin or cutaneous origin. As such, the HSV1 replication in the host cell ge- fined, shallow, round or oval lesions with
following the rupture of the herpes labia- nome on an enzymatic level. With ‘cold a necrotic fibrinous center covered with a
lis vesicles, the lesion will go through the sores’ the host cells affected are in the yellow-grayish pseudomembrane and sur-
following stages: soft crust, hard crust, stratified squamous epithelium of the ver- rounded by an erythematous halo. Minor
then scab. It is important to remember that milion border of the lip. Without treatment aphthous ulcers are less than one centime-
the patient is contagious through the scab secondary herpetic lesions will resolve on ter in size, last 7 to 10 days, and only occur
stage and they should be aware that they their own, typically within 8 to 10 days. on the movable oral mucosa, labial mucosa,
could transmit the virus to others (Figures They are self-limiting. However, the goal buccal mucosa, tongue, floor of mouth and
11-17). Regardless of whether the patient of treatment is to reduce the severity of soft palate. They resolve on their own with-
out treatment and heal without scarring.
They are quite common, often presenting
with more than one ulcer and are far more
painful than they should be for their size
(Figures 18- 20).
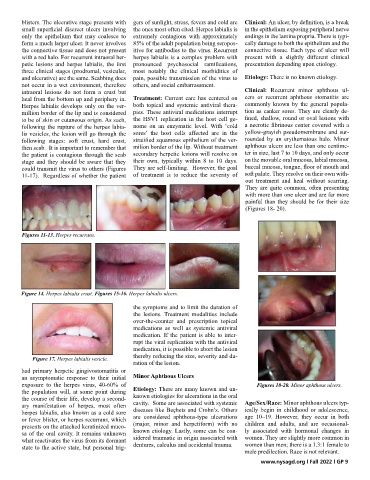
Figures 11-13. Herpes recurrans.
Figure 14. Herpes labialis crust. Figures 15-16. Herpes labialis ulcers.
the symptoms and to limit the duration of
the lesions. Treatment modalities include
over-the-counter and prescription topical
medications as well as systemic antiviral
medication. If the patient is able to inter-
rupt the viral replication with the antiviral
medication, it is possible to abort the lesion
thereby reducing the size, severity and du-
Figure 17. Herpes labialis vesicle.
ration of the lesion.
had primary herpetic gingivostomatitis or
an asymptomatic response to their initial Minor Aphthous Ulcers
exposure to the herpes virus, 40-60% of Figures 18-20. Minor aphthous ulcers.
the population will, at some point during Etiology: There are many known and un-
the course of their life, develop a second- known etiologies for ulcerations in the oral
ary manifestation of herpes, most often cavity. Some are associated with systemic Age/Sex/Race: Minor aphthous ulcers typ-
herpes labialis, also known as a cold sore diseases like Beçhets and Crohn’s. Others ically begin in childhood or adolescence,
or fever blister, or herpes recurrans, which are considered aphthous-type ulcerations age 10–19. However, they occur in both
presents on the attached keratinized muco- (major, minor and herpetiform) with no children and adults, and are occasional-
sa of the oral cavity. It remains unknown known etiology. Lastly, some can be con- ly associated with hormonal changes in
what reactivates the virus from its dormant sidered traumatic in origin associated with women. They are slightly more common in
state to the active state, but personal trig- dentures, calculus and accidental trauma. women than men; there is a 1.3:1 female to
male predilection. Race is not relevant.
www.nysagd.org l Fall 2022 l GP 9