
Page 30 - GP Fall 2020
P. 30
the hyperplastic peri-implant tissues was ation in gingival connective tissue homeo- ity of drug induced gingival hyperplasia.
8
sent for histopathologic evaluation. The bi- stasis, inflammatory changes, and direct ac- The interaction between the drug and gin-
opsy report revealed epithelial cells and fi- tion of medications on growth factors. gival tissues could be enhanced by gingival
brous hyperplasia, consistent with gingival inflammation caused by poor oral hygiene.
hyperplasia. Gingival hyperplasia may appear as a firm, It has also been documented that, upon dis-
nodular enlargement of the interdental continuation of these drugs, gingival en-
The patient was referred back to her cardi- papillae, and its prevalence in the mouth is largement may be reduced within one week.
ologist for a re-evaluation with regards to varied. It affects the anterior more than the If the hyperplastic gingival tissue does not
the usage of OM-HCTZ and recommen- posterior and are more pronounced on the respond to plaque control or scaling and
dations for discontinuation or changing to facial than the lingual gingival surfaces of root planning, it needs to be excised.
a different medication due to the develop- teeth or implants (Figures 5, 6, 7).
ment of gingival hyperplasia and possible Discontinuation of the related medication
risk of peri-implantitis. The cardiologist has been shown to reduce gingival over-
recommended that the patient continue OM- growth; however, the growth will recur
HCTZ since she was unable to tolerate or when the medication is readministered . In
4
control her blood pressure with other hyper- cases where alternative medications can be
tensives. used, substitution of the related drug has
been shown to result in regression of the
Fortunately, this did not interfere with pa- overgrowth. In this case report it was found
tient home care and therefore surgical cor- that the amlodipine was not well tolerated
rection for the hyperplastic tissue was not and when she began taking OM-HCTZ, she
performed. Additionally, the patient has a developed gingival hyperplasia. Maintain-
low smile line and there was no complaint ing adequate blood pressure control can-
regarding her esthetics. The subsequent not be compromised and thus measures at
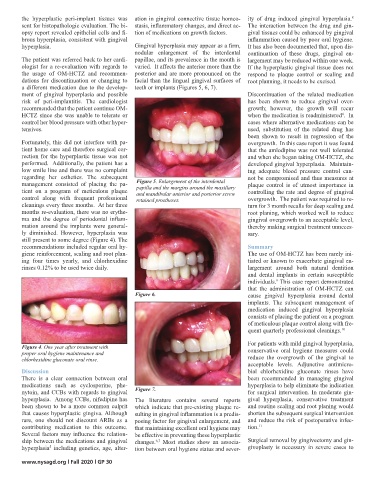
management consisted of placing the pa- Figure 5. Enlargement of the interdental plaque control is of utmost importance in
papilla and the margins around the maxillary
tient on a program of meticulous plaque and mandibular anterior and posterior screw controlling the rate and degree of gingival
control along with frequent professional retained prostheses. overgrowth. The patient was required to re-
cleanings every three months. At her three turn for 3 month recalls for deep scaling and
months re-evaluation, there was no erythe- root planing, which worked well to reduce
ma and the degree of periodontal inflam- gingival overgrowth to an acceptable level,
mation around the implants were general- thereby making surgical treatment unneces-
ly diminished. However, hyperplasia was sary.
still present to some degree (Figure 4). The
recommendations included regular oral hy- Summary
giene reinforcement, scaling and root plan- The use of OM-HCTZ has been rarely ini-
ing four times yearly, and chlorhexidine tiated or known to exacerbate gingival en-
rinses 0.12% to be used twice daily. largement around both natural dentition
and dental implants in certain susceptible
individuals. This case report demonstrated
9
that the administration of OM-HCTZ can
Figure 6. cause gingival hyperplasia around dental
implants. The subsequent management of
medication induced gingival hyperplasia
consists of placing the patient on a program
of meticulous plaque control along with fre-
quent quarterly professional cleanings. 10
For patients with mild gingival hyperplasia,
Figure 4. One year after treatment with conservative oral hygiene measures could
proper oral hygiene maintenance and
chlorhexidine gluconate oral rinse. reduce the overgrowth of the gingival to
acceptable levels. Adjunctive antimicro-
Discussion bial chlorhexidine gluconate rinses have
There is a clear connection between oral been recommended in managing gingival
medications such as cyclosporine, phe- hyperplasia to help eliminate the indication
nytoin, and CCBs with regards to gingival Figure 7. for surgical intervention. In moderate gin-
hyperplasia. Among CCBs, nifedipine has The literature contains several reports gival hyperplasia, conservative treatment
been shown to be a more common culprit which indicate that pre-existing plaque re- and routine scaling and root planing would
that causes hyperplastic gingiva. Although sulting in gingival inflammation is a predis- shorten the subsequent surgical intervention
rare, one should not discount ARBs as a posing factor for gingival enlargement, and and reduce the risk of postoperative infec-
contributing medication to this outcome. that maintaining excellent oral hygiene may tion. 11
Several factors may influence the relation- be effective in preventing these hyperplastic
ship between the medications and gingival changes. Most studies show an associa- Surgical removal by gingivectomy and gin-
6,7
hyperplasia including genetics, age, alter- tion between oral hygiene status and sever- givoplasty is necessary in severe cases to
5
www.nysagd.org l Fall 2020 l GP 30