
Page 9 - ABC - Tech BG_1A
P. 9
Medical Plan Choices | California 7
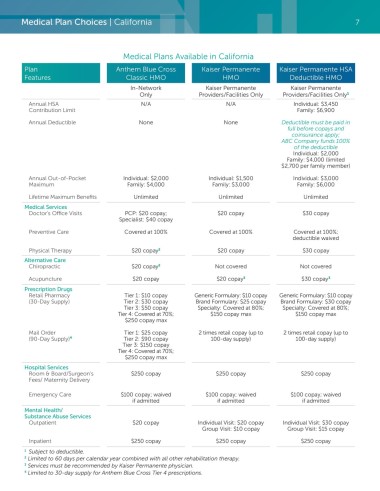
Medical Plans Available in California
Plan Anthem Blue Cross Kaiser Permanente Kaiser Permanente HSA
Features Classic HMO HMO Deductible HMO
In-Network Kaiser Permanente Kaiser Permanente
Only Providers/Facilities Only Providers/Facilities Only 1
Annual HSA N/A N/A Individual: $3,450
Contribution Limit Family: $6,900
Annual Deductible None None Deductible must be paid in
full before copays and
coinsurance apply;
ABC Company funds 100%
of the deductible
Individual: $2,000
Family: $4,000 (limited
$2,700 per family member)
Annual Out-of-Pocket Individual: $2,000 Individual: $1,500 Individual: $3,000
Maximum Family: $4,000 Family: $3,000 Family: $6,000
Lifetime Maximum Benefits Unlimited Unlimited Unlimited
Medical Services
Doctor’s Office Visits PCP: $20 copay; $20 copay $30 copay
Specialist: $40 copay
Preventive Care Covered at 100% Covered at 100% Covered at 100%;
deductible waived
Physical Therapy $20 copay 2 $20 copay $30 copay
Alternative Care
Chiropractic $20 copay 2 Not covered Not covered
Acupuncture $20 copay $20 copay 3 $30 copay 3
Prescription Drugs
Retail Pharmacy Tier 1: $10 copay Generic Formulary: $10 copay Generic Formulary: $10 copay
(30-Day Supply) Tier 2: $30 copay Brand Formulary: $25 copay Brand Formulary: $30 copay
Tier 3: $50 copay Specialty: Covered at 80%; Specialty: Covered at 80%;
Tier 4: Covered at 70%; $150 copay max $150 copay max
$250 copay max
Mail Order Tier 1: $25 copay 2 times retail copay (up to 2 times retail copay (up to
(90-Day Supply) 4 Tier 2: $90 copay 100-day supply) 100-day supply)
Tier 3: $150 copay
Tier 4: Covered at 70%;
$250 copay max
Hospital Services
Room & Board/Surgeon’s $250 copay $250 copay $250 copay
Fees/ Maternity Delivery
Emergency Care $100 copay; waived $100 copay; waived $100 copay; waived
if admitted if admitted if admitted
Mental Health/
Substance Abuse Services
Outpatient $20 copay Individual Visit: $20 copay Individual Visit: $30 copay
Group Visit: $10 copay Group Visit: $15 copay
Inpatient $250 copay $250 copay $250 copay
1 Subject to deductible.
2 Limited to 60 days per calendar year combined with all other rehabilitation therapy.
3 Services must be recommended by Kaiser Permanente physician.
4 Limited to 30-day supply for Anthem Blue Cross Tier 4 prescriptions.