
Page 7 - Casting Network Benefits Guide 2020
P. 7
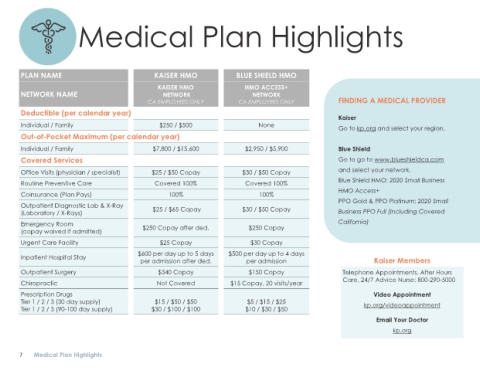
Medical Plan Highlights
PLAN NAME KAISER HMO BLUE SHIELD HMO
KAISER HMO HMO ACCESS+
NETWORK NAME NETWORK NETWORK
CA EMPLOYEES ONLY CA EMPLOYEES ONLY FINDING A MEDICAL PROVIDER
Deductible (per calendar year)
Kaiser
Individual / Family $250 / $500 None Go to kp.org and select your region.
Out-of-Pocket Maximum (per calendar year)
Individual / Family $7,800 / $15,600 $2,950 / $5,900 Blue Shield
Covered Services Go to go to www.blueshieldca.com
Office Visits (physician / specialist) $25 / $50 Copay $30 / $50 Copay and select your network.
Routine Preventive Care Covered 100% Covered 100% Blue Shield HMO: 2020 Small Business
HMO Access+
Coinsurance (Plan Pays) 100% 100%
PPO Gold & PPO Platinum: 2020 Small
Outpatient Diagnostic Lab & X-Ray $25 / $65 Copay $30 / $50 Copay
(Laboratory / X-Rays) Business PPO Full (Including Covered
Emergency Room $250 Copay after ded. $250 Copay California)
(copay waived if admitted)
Urgent Care Facility $25 Copay $30 Copay
$600 per day up to 5 days $500 per day up to 4 days
Inpatient Hospital Stay
per admission after ded. per admission Kaiser Members
Outpatient Surgery $340 Copay $150 Copay Telephone Appointments, After Hours
Care, 24/7 Advice Nurse: 800-290-5000
Chiropractic Not Covered $15 Copay, 20 visits/year
Prescription Drugs Video Appointment
Tier 1 / 2 / 3 (30 day supply) $15 / $50 / $50 $5 / $15 / $25 kp.org/videoappointment
Tier 1 / 2 / 3 (90-100 day supply) $30 / $100 / $100 $10 / $30 / $50
Email Your Doctor
kp.org
7 Medical Plan Highlights