
Page 10 - Casting Network Benefits Guide 2020
P. 10
Dental Vision
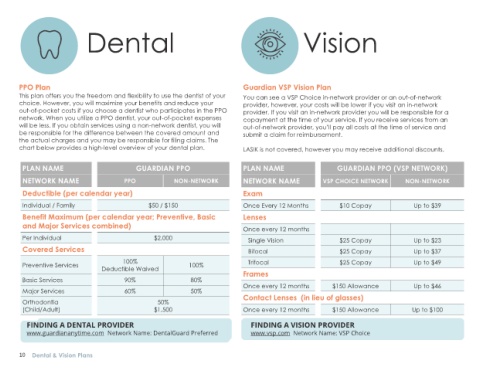
PPO Plan Guardian VSP Vision Plan
This plan offers you the freedom and flexibility to use the dentist of your You can see a VSP Choice in-network provider or an out-of-network
choice. However, you will maximize your benefits and reduce your provider, however, your costs will be lower if you visit an in-network
out-of-pocket costs if you choose a dentist who participates in the PPO provider. If you visit an in-network provider you will be responsible for a
network. When you utilize a PPO dentist, your out-of-pocket expenses copayment at the time of your service. If you receive services from an
will be less. If you obtain services using a non-network dentist, you will out-of-network provider, you’ll pay all costs at the time of service and
be responsible for the difference between the covered amount and submit a claim for reimbursement.
the actual charges and you may be responsible for filing claims. The
chart below provides a high-level overview of your dental plan. LASIK is not covered, however you may receive additional discounts.
PLAN NAME GUARDIAN PPO PLAN NAME GUARDIAN PPO (VSP NETWORK)
NETWORK NAME PPO NON-NETWORK NETWORK NAME VSP CHOICE NETWORK NON-NETWORK
Deductible (per calendar year) Exam
Individual / Family $50 / $150 Once Every 12 Months $10 Copay Up to $39
Benefit Maximum (per calendar year; Preventive, Basic Lenses
and Major Services combined) Once every 12 months
Per Individual $2,000 Single Vision $25 Copay Up to $23
Covered Services Bifocal $25 Copay Up to $37
100% Trifocal $25 Copay Up to $49
Preventive Services 100%
Deductible Waived
Frames
Basic Services 90% 80%
Once every 12 months $150 Allowance Up to $46
Major Services 60% 50%
Contact Lenses (in lieu of glasses)
Orthodontia 50%
(Child/Adult) $1,500 Once every 12 months $150 Allowance Up to $100
FINDING A DENTAL PROVIDER FINDING A VISION PROVIDER
www.guardiananytime.com Network Name: DentalGuard Preferred www.vsp.com Network Name: VSP Choice
10 Dental & Vision Plans