
Page 8 - Casting Network Benefits Guide 2020
P. 8
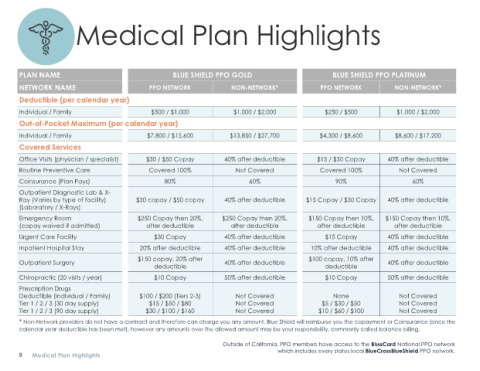
Medical Plan Highlights
PLAN NAME BLUE SHIELD PPO GOLD BLUE SHIELD PPO PLATINUM
NETWORK NAME PPO NETWORK NON-NETWORK* PPO NETWORK NON-NETWORK*
Deductible (per calendar year)
Individual / Family $500 / $1,000 $1,000 / $2,000 $250 / $500 $1,000 / $2,000
Out-of-Pocket Maximum (per calendar year)
Individual / Family $7,800 / $15,600 $13,850 / $27,700 $4,300 / $8,600 $8,600 / $17,200
Covered Services
Office Visits (physician / specialist) $30 / $50 Copay 40% after deductible $15 / $30 Copay 40% after deductible
Routine Preventive Care Covered 100% Not Covered Covered 100% Not Covered
Coinsurance (Plan Pays) 80% 60% 90% 60%
Outpatient Diagnostic Lab & X-
Ray (Varies by type of facility) $30 copay / $50 copay 40% after deductible $15 Copay / $30 Copay 40% after deductible
(Laboratory / X-Rays)
Emergency Room $250 Copay then 20%, $250 Copay then 20%, $150 Copay then 10%, $150 Copay then 10%,
(copay waived if admitted) after deductible after deductible after deductible after deductible
Urgent Care Facility $30 Copay 40% after deductible $15 Copay 40% after deductible
Inpatient Hospital Stay 20% after deductible 40% after deductible 10% after deductible 40% after deductible
$150 copay, 20% after $100 copay, 10% after
Outpatient Surgery 40% after deductible 40% after deductible
deductible deductible
Chiropractic (20 visits / year) $10 Copay 50% after deductible $10 Copay 50% after deductible
Prescription Drugs
Deductible (Individual / Family) $100 / $200 (Tiers 2-3) Not Covered None Not Covered
Tier 1 / 2 / 3 (30 day supply) $15 / $50 / $80 Not Covered $5 / $30 / $50 Not Covered
Tier 1 / 2 / 3 (90 day supply) $30 / $100 / $160 Not Covered $10 / $60 / $100 Not Covered
* Non-Network providers do not have a contract and therefore can charge you any amount. Blue Shield will reimburse you the copayment or Coinsurance (once the
calendar year deductible has been met), however any amounts over the allowed amount may be your responsibility, commonly called balance billing.
Outside of California, PPO members have access to the BlueCard National PPO network
which includes every states local BlueCrossBlueShield PPO network.
8 Medical Plan Highlights