
Page 159 - Essential Haematology
P. 159
Chapter 10 Spleen / 145
(a) (b)
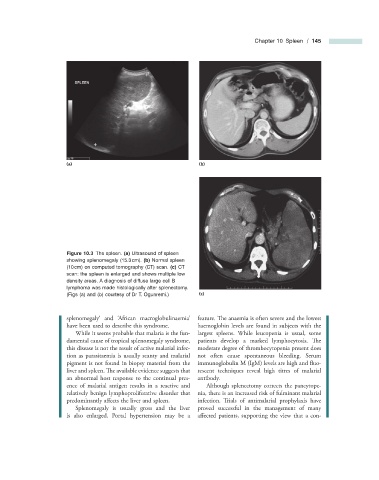
Figure 10.3 The spleen. (a) Ultrasound of spleen
showing splenomegaly (15.3 cm). (b) Normal spleen
(10 cm) on computed tomography (CT) scan. (c) CT
scan: the spleen is enlarged and shows multiple low
density areas. A diagnosis of diffuse large cell B
lymphoma was made histologically after splenectomy.
(Figs (a) and (b) courtesy of Dr T. Ogunremi.) (c)
splenomegaly ’ and ‘ African macroglobulinaemia ’ feature. The anaemia is often severe and the lowest
have been used to describe this syndrome. haemoglobin levels are found in subjects with the
While it seems probable that malaria is the fun- largest spleens. While leucopenia is usual, some
damental cause of tropical splenomegaly syndrome, patients develop a marked lymphocytosis. Th e
this disease is not the result of active malarial infec- moderate degree of thrombocytopenia present does
tion as parasitaemia is usually scanty and malarial not often cause spontaneous bleeding. Serum
pigment is not found in biopsy material from the immunoglobulin M (IgM) levels are high and fl uo-
liver and spleen. The available evidence suggests that rescent techniques reveal high titres of malarial
an abnormal host response to the continual pres- antibody.
ence of malarial antigen results in a reactive and Although splenectomy corrects the pancytope-
relatively benign lymphoproliferative disorder that nia, there is an increased risk of fulminant malarial
predominantly affects the liver and spleen. infection. Trials of antimalarial prophylaxis have
Splenomegaly is usually gross and the liver proved successful in the management of many
is also enlarged. Portal hypertension may be a affected patients, supporting the view that a con-