
Page 226 - Essential Haematology
P. 226
212 / Chapter 15 Myeloproliferative neoplasms
Mastocytosis
Mastocytosis is a clonal neoplastic proliferation of
mast cells that accumulate in one or more organ
systems. Mast cells (tissue basophils) are derived
from haemopoietic stem cells. Mature cells survive
for months or years in vascular tissues and most
organs. Systemic mastocytosis is a clonal myelopro-
liferative disorder involving usually the bone
marrow, heart, spleen, lymph nodes and skin.
The somatic KIT mutation Asp816Val is
detected in the majority of patients and may be
partly responsible for autonomous growth and
enhanced survival of the neoplastic mast cells. In
many patients this mutation is also detected in
other haemopoietic cells.
Symptoms are related to histamine and prostag-
landin release and include fl ushing, pruritus,
abdominal pain and bronchospasm. H 1 and H 2
antihistamine blocking drugs are valuable. Th e skin
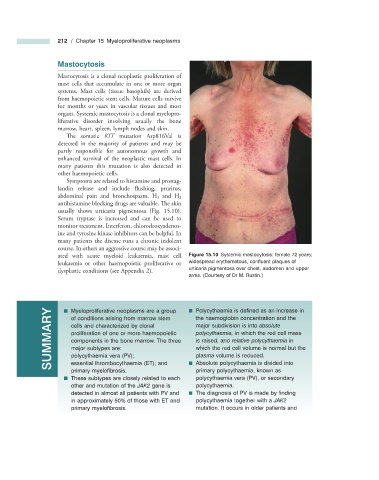
usually shows urticaria pigmentosa (Fig. 15.10 ).
Serum tryptase is increased and can be used to
monitor treatment. Interferon, chlorodeoxyadenos-
ine and tyrosine kinase inhibitors can be helpful. In
many patients the disease runs a chronic indolent
course. In others an aggressive course may be associ-
ated with acute myeloid leukaemia, mast cell Figure 15.10 Systemic mastocytosis: female 72 years;
leukaemia or other haemopoietic proliferative or widespread erythematous, confl uent plaques of
dysplastic conditions (see Appendix 2 ). urticaria pigmentosa over chest, abdomen and upper
arms. (Courtesy of Dr M. Rustin.)
SUMMARY ■ Myeloproliferative neoplasms are a group ■ Polycythaemia is defi ned as an increase in
of conditions arising from marrow stem
the haemoglobin concentration and the
major subdivision is into absolute
cells and characterized by clonal
polycythaemia, in which the red cell mass
proliferation of one or more haemopoietic
is raised, and relative polycythaemia in
components in the bone marrow. The three
which the red cell volume is normal but the
major subtypes are:
plasma volume is reduced.
polycythaemia vera (PV);
essential thrombocythaemia (ET); and
primary myelofi brosis. ■ Absolute polycythaemia is divided into
primary polycythaemia, known as
■ These subtypes are closely related to each polycythaemia vera (PV), or secondary
other and mutation of the JAK2 gene is polycythaemia.
detected in almost all patients with PV and ■ The diagnosis of PV is made by fi nding
in approximately 50% of those with ET and polycythaemia together with a JAK2
primary myelofi brosis. mutation. It occurs in older patients and