
Page 7 - Watkins Associated Industries, Inc - 2022 Benefits Guide
P. 7
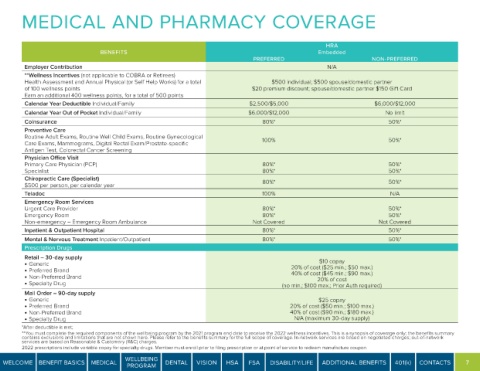
MEDICAL AND PHARMACY COVERAGE
HRA
BENEFITS Embedded
PREFERRED NON-PREFERRED
Employer Contribution N/A
**Wellness Incentives (not applicable to COBRA or Retirees)
Health Assessment and Annual Physical (or Self Help Works) for a total $500 individual; $500 spouse/domestic partner
of 100 wellness points $20 premium discount; spouse/domestic partner $150 Gift Card
Earn an additional 400 wellness points, for a total of 500 points
Calendar Year Deductible Individual/Family $2,500/$5,000 $6,000/$12,000
Calendar Year Out of Pocket Individual/Family $6,000/$12,000 No limit
Coinsurance 80%* 50%*
Preventive Care
Routine Adult Exams, Routine Well Child Exams, Routine Gynecological
Care Exams, Mammograms, Digital Rectal Exam/Prostate-specific 100% 50%*
Antigen Test, Colorectal Cancer Screening
Physician Office Visit
Primary Care Physician (PCP) 80%* 50%*
Specialist 80%* 50%*
Chiropractic Care (Specialist)
$500 per person, per calendar year 80%* 50%*
Teladoc 100% N/A
Emergency Room Services
Urgent Care Provider 80%* 50%*
Emergency Room 80%* 50%*
Non-emergency – Emergency Room Ambulance Not Covered Not Covered
Inpatient & Outpatient Hospital 80%* 50%*
Mental & Nervous Treatment Inpatient/Outpatient 80%* 50%*
Prescription Drugs
Retail – 30-day supply
• Generic $10 copay
• Preferred Brand 20% of cost ($25 min.; $50 max.)
40% of cost ($45 min.; $90 max.)
• Non-Preferred Brand 20% of cost
• Specialty Drug (no min.; $100 max.; Prior Auth required)
Mail Order – 90-day supply
• Generic $25 copay
• Preferred Brand 20% of cost ($50 min.; $100 max.)
• Non-Preferred Brand 40% of cost ($90 min.; $180 max.)
• Specialty Drug N/A (maximum 30-day supply)
*After deductible is met;
**You must complete the required components of the wellbeing program by the 2021 program end date to receive the 2022 wellness incentives. This is a synopsis of coverage only; the benefits summary
contains exclusions and limitations that are not shown here. Please refer to the benefits summary for the full scope of coverage. In-network services are based on negotiated charges; out-of-network
services are based on Reasonable & Customary (R&C) charges.
2022 prescriptions include variable copay for specialty drugs. Member must enroll prior to filing prescription or at point of service to redeem manufacture coupon.
WELLBEING
WELCOME BENEFIT BASICS MEDICAL DENTAL VISION HSA FSA DISABILITY/LIFE ADDITIONAL BENEFITS 401(k) CONTACTS 7
PROGRAM