
Page 8 - Watkins Associated Industries, Inc - 2022 Benefits Guide
P. 8
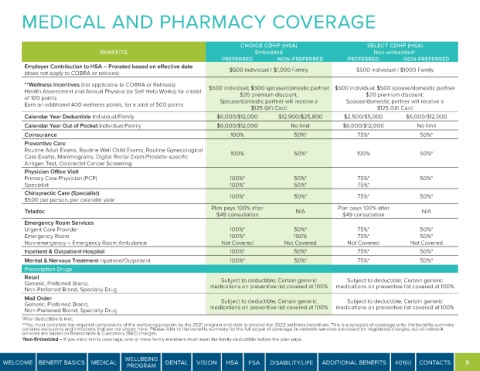
MEDICAL AND PHARMACY COVERAGE
CHOICE CDHP (HSA) SELECT CDHP (HSA)
BENEFITS Embedded Non-embedded†
PREFERRED NON-PREFERRED PREFERRED NON-PREFERRED
Employer Contribution to HSA – Prorated based on effective date
(does not apply to COBRA or retirees) $500 Individual / $1,000 Family $500 individual / $1000 Family
**Wellness Incentives (not applicable to COBRA or Retirees)
Health Assessment and Annual Physical (or Self Help Works) for a total $500 individual; $500 spouse/domestic partner $500 individual; $500 spouse/domestic partner
of 100 points $20 premium discount; $20 premium discount;
Earn an additional 400 wellness points, for a total of 500 points Spouse/domestic partner will receive a Spouse/domestic partner will receive a
$125 Gift Card $125 Gift Card
Calendar Year Deductible Individual/Family $6,000/$12,000 $12,900/$25,800 $2,500/$5,000 $6,000/$12,000
Calendar Year Out of Pocket Individual/Family $6,000/$12,000 No limit $6,000/$12,000 No limit
Coinsurance 100% 50%* 75%* 50%*
Preventive Care
Routine Adult Exams, Routine Well Child Exams, Routine Gynecological
Care Exams, Mammograms, Digital Rectal Exam/Prostate-specific 100% 50%* 100% 50%*
Antigen Test, Colorectal Cancer Screening
Physician Office Visit
Primary Care Physician (PCP) 100%* 50%* 75%* 50%*
Specialist 100%* 50%* 75%*
Chiropractic Care (Specialist)
$500 per person, per calendar year 100%* 50%* 75%* 50%*
Teladoc Plan pays 100% after N/A Plan pays 100% after N/A
$49 consultation $49 consultation
Emergency Room Services
Urgent Care Provider 100%* 50%* 75%* 50%*
Emergency Room 100%* 100% 75%* 50%*
Non-emergency – Emergency Room Ambulance Not Covered Not Covered Not Covered Not Covered
Inpatient & Outpatient Hospital 100%* 50%* 75%* 50%*
Mental & Nervous Treatment Inpatient/Outpatient 100%* 50%* 75%* 50%*
Prescription Drugs
Retail Subject to deductible; Certain generic Subject to deductible; Certain generic
Generic, Preferred Brand, medications on preventive list covered at 100% medications on preventive list covered at 100%
Non-Preferred Brand, Specialty Drug
Mail Order
Subject to deductible; Certain generic
Subject to deductible; Certain generic
Generic, Preferred Brand, medications on preventive list covered at 100% medications on preventive list covered at 100%
Non-Preferred Brand, Specialty Drug
*After deductible is met;
**You must complete the required components of the wellbeing program by the 2021 program end date to receive the 2022 wellness incentives. This is a synopsis of coverage only; the benefits summary
contains exclusions and limitations that are not shown here. Please refer to the benefits summary for the full scope of coverage. In-network services are based on negotiated charges; out-of-network
services are based on Reasonable & Customary (R&C) charges.
†Non-Embedded – If you elect family coverage, one or more family members must meet the family deductible before the plan pays.
WELLBEING
WELCOME BENEFIT BASICS MEDICAL DENTAL VISION HSA FSA DISABILITY/LIFE ADDITIONAL BENEFITS 401(k) CONTACTS 8
PROGRAM