
Page 6 - Genesis Care 2022 Benefit Guide
P. 6
Medical & Spending Voluntary Additional
Contents Prescription Dental Vision Accounts Life & AD&D Disability Benefits 401(k) Information Contacts
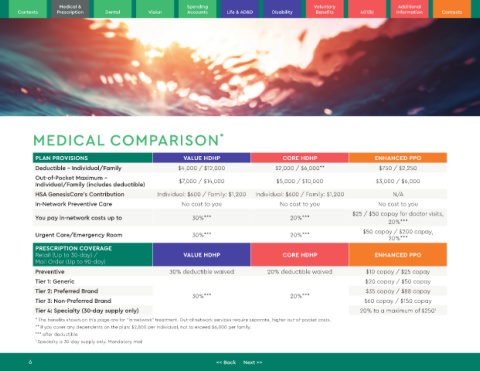
MEDICAL COMPARISON *
PLAN PROVISIONS VALUE HDHP CORE HDHP ENHANCED PPO
Deductible - Individual/Family $4,000 / $12,000 $2,000 / $6,000** $750 / $2,250
Out-of-Pocket Maximum – $7,000 / $14,000 $5,000 / $10,000 $3,000 / $6,000
Individual/Family (includes deductible)
HSA GenesisCare’s Contribution Individual: $600 / Family: $1,200 Individual: $600 / Family: $1,200 N/A
In-Network Preventive Care No cost to you No cost to you No cost to you
$25 / $50 copay for doctor visits,
You pay in-network costs up to 30%*** 20%***
20%***
$50 copay / $200 copay,
Urgent Care/Emergency Room 30%*** 20%***
20%***
PRESCRIPTION COVERAGE
Retail (Up to 30-day) / VALUE HDHP CORE HDHP ENHANCED PPO
Mail Order (Up to 90-day)
Preventive 30% deductible waived 20% deductible waived $10 copay / $25 copay
Tier 1: Generic $20 copay / $50 copay
Tier 2: Preferred Brand 30%*** 20%*** $35 copay / $88 copay
Tier 3: Non-Preferred Brand $60 copay / $150 copay
Tier 4: Specialty (30-day supply only) 20% to a maximum of $250 1
* The benefits shown on this page are for "in-network" treatment. Out-of network services require separate, higher out-of-pocket costs.
** If you cover any dependents on the plan: $2,800 per individual, not to exceed $6,000 per family.
*** after deductible
1 Specialty is 30-day supply only. Mandatory mail
6 << Back Next >>