
Page 18 - HutsonWood-2023-24-Benefit Guide
P. 18
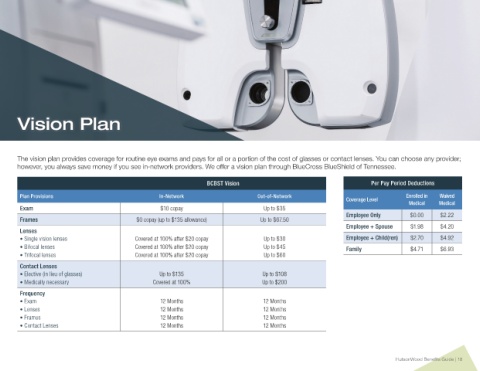
Vision Plan
The vision plan provides coverage for routine eye exams and pays for all or a portion of the cost of glasses or contact lenses. You can choose any provider;
however, you always save money if you see in-network providers. We offer a vision plan through BlueCross BlueShield of Tennessee.
BCBST Vision Per Pay Period Deductions
Plan Provisions In-Network Out-of-Network Enrolled in Waived
Coverage Level
Medical Medical
Exam $10 copay Up to $35
Employee Only $0.00 $2.22
Frames $0 copay (up to $135 allowance) Up to $67.50
Employee + Spouse $1.98 $4.20
Lenses
• Single vision lenses Covered at 100% after $20 copay Up to $30 Employee + Child(ren) $2.70 $4.92
• Bifocal lenses Covered at 100% after $20 copay Up to $45 Family $4.71 $6.93
• Trifocal lenses Covered at 100% after $20 copay Up to $60
Contact Lenses
• Elective (in lieu of glasses) Up to $135 Up to $108
• Medically necessary Covered at 100% Up to $200
Frequency
• Exam 12 Months 12 Months
• Lenses 12 Months 12 Months
• Frames 12 Months 12 Months
• Contact Lenses 12 Months 12 Months
HutsonWood Benefits Guide | 18