
Page 11 - 2022 New Relic Guide
P. 11
Summary of Your Your Health Pre-Tax Spending Life/AD&D Where to Find
Dental & Vision
How to Get Started Dental & Vision 401(k) Additional Benefits
Contributions Benefits Accounts Disability Support
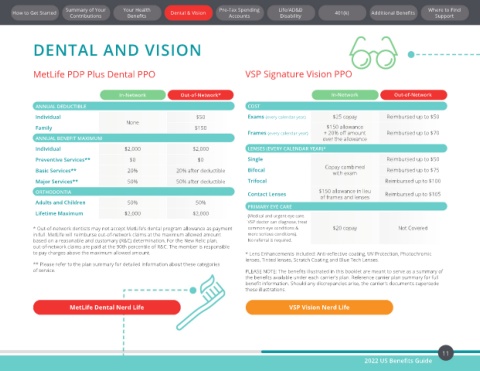
DENTAL AND VISION
MetLife PDP Plus Dental PPO VSP Signature Vision PPO
In-Network Out-of-Network* In-Network Out-of-Network
ANNUAL DEDUCTIBLE COST
Individual $50 Exams (every calendar year) $25 copay Reimbursed up to $50
None
Family $150 $150 allowance
Frames (every calendar year) + 20% off amount Reimbursed up to $70
ANNUAL BENEFIT MAXIMUM over the allowance
Individual $2,000 $2,000 LENSES (EVERY CALENDAR YEAR)*
Preventive Services** $0 $0 Single Reimbursed up to $50
Copay combined
Basic Services** 20% 20% after deductible Bifocal with exam Reimbursed up to $75
Major Services** 50% 50% after deductible Trifocal Reimbursed up to $100
ORTHODONTIA Contact Lenses $150 allowance in lieu Reimbursed up to $105
of frames and lenses
Adults and Children 50% 50%
PRIMARY EYE CARE
Lifetime Maximum $2,000 $2,000 (Medical and urgent eye care.
VSP doctor can diagnose, treat
* Out-of-network dentists may not accept MetLife’s dental program allowance as payment common eye conditions & $20 copay Not Covered
in full. MetLife will reimburse out-of-network claims at the maximum allowed amount more serious conditions).
based on a reasonable and customary (R&C) determination. For the New Relic plan, No referral is required.
out-of-network claims are paid at the 90th percentile of R&C. The member is responsible
to pay charges above the maximum allowed amount. * Lens Enhancements included: Anti-reflective coating, UV Protection, Photochromic
lenses, Tinted lenses, Scratch Coating and Blue Tech Lenses.
** Please refer to the plan summary for detailed information about these categories
of service. PLEASE NOTE: The benefits illustrated in this booklet are meant to serve as a summary of
the benefits available under each carrier's plan. Reference carrier plan summary for full
benefit information. Should any discrepancies arise, the carrier's documents supersede
these illustrations.
MetLife Dental Nerd Life VSP Vision Nerd Life
11
2022 US Benefits Guide