
Page 9 - 2022 New Relic Guide
P. 9
Summary of Your Your Health Pre-Tax Spending Life/AD&D Where to Find
Your Health
How to Get Started Dental & Vision 401(k) Additional Benefits
Contributions BenefitsBenefits Accounts Disability Support
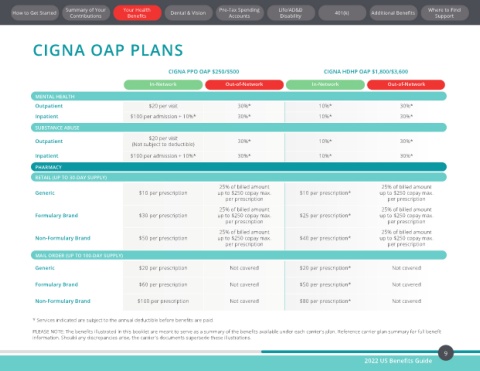
CIGNA OAP PLANS
CIGNA PPO OAP $250/$500 CIGNA HDHP OAP $1,800/$3,600
In-Network Out-of-Network In-Network Out-of-Network
MENTAL HEALTH
Outpatient $20 per visit 30%* 10%* 30%*
Inpatient $100 per admission + 10%* 30%* 10%* 30%*
SUBSTANCE ABUSE
$20 per visit
Outpatient 30%* 10%* 30%*
(Not subject to deductible)
Inpatient $100 per admission + 10%* 30%* 10%* 30%*
PHARMACY
RETAIL (UP TO 30-DAY SUPPLY)
25% of billed amount 25% of billed amount
Generic $10 per prescription up to $250 copay max. $10 per prescription* up to $250 copay max.
per prescription per prescription
25% of billed amount 25% of billed amount
Formulary Brand $30 per prescription up to $250 copay max. $25 per prescription* up to $250 copay max.
per prescription per prescription
25% of billed amount 25% of billed amount
Non-Formulary Brand $50 per prescription up to $250 copay max. $40 per prescription* up to $250 copay max.
per prescription per prescription
MAIL ORDER (UP TO 100-DAY SUPPLY)
Generic $20 per prescription Not covered $20 per prescription* Not covered
Formulary Brand $60 per prescription Not covered $50 per prescription* Not covered
Non-Formulary Brand $100 per prescription Not covered $80 per prescription* Not covered
* Services indicated are subject to the annual deductible before benefits are paid.
PLEASE NOTE: The benefits illustrated in this booklet are meant to serve as a summary of the benefits available under each carrier's plan. Reference carrier plan summary for full benefit
information. Should any discrepancies arise, the carrier's documents supersede these illustrations.
9
2022 US Benefits Guide