
Page 44 - DP Vol 20 No 5_Neat
P. 44
IMPLANTOLOGY SECTION
DS PRIMETAPER IMPLANT SYSTEM
FOR SMILE REHABILITATION:
A CLINICAL PERSPECTIVE
Gaurav Gupta, D.K. Gupta, Neelja Gupta
INTRODUCTION
Missing teeth can compromise esthetics, mastication, and speech.
Dental implants are the most widely used fixed restorations for partially
or completely edentulous patients, with survival rates exceeding 90%
due to their functional and aesthetic benefits . This is particularly
[1]
advantageous for the anterior maxilla, a region highly sensitive to
appearance. Studies indicate that outcomes from this approach are
comparable to those achieved with traditional implant placement and
restoration protocols [2, 3] .
Factors influencing primary stability include bone quality and
quantity, surgical techniques, and implant design .
[4]
Tapered implants create tight contact between the osteotomy wall
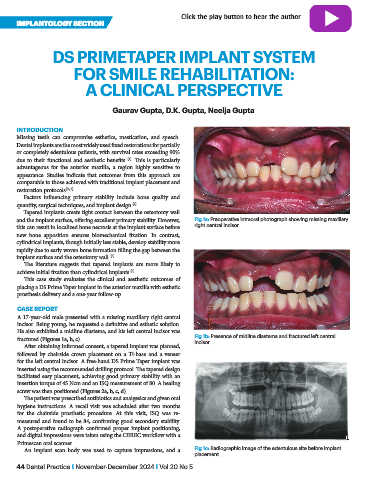
and the implant surface, offering excellent primary stability. However, Fig 1a: Preoperative intraoral photograph showing missing maxillary
this can result in localized bone necrosis at the implant surface before right central incisor.
new bone apposition ensures biomechanical fixation. In contrast,
cylindrical implants, though initially less stable, develop stability more
rapidly due to early woven bone formation filling the gap between the
implant surface and the osteotomy wall .
[5]
The literature suggests that tapered implants are more likely to
achieve initial fixation than cylindrical implants .
[6]
This case study evaluates the clinical and aesthetic outcomes of
placing a DS Prime Taper implant in the anterior maxilla with esthetic
prosthesis delivery and a one-year follow-up.
CASE REPORT
A 17-year-old male presented with a missing maxillary right central
incisor. Being young, he requested a definitive and esthetic solution.
He also exhibited a midline diastema, and his left central incisor was
fractured (Figures 1a, b, c). Fig 1b: Presence of midline diastema and fractured left central
After obtaining informed consent, a tapered implant was planned, incisor.
followed by chairside crown placement on a Ti-base and a veneer
for the left central incisor. A free-hand DS Prime Taper implant was
inserted using the recommended drilling protocol. The tapered design
facilitated easy placement, achieving good primary stability with an
insertion torque of 45 Ncm and an ISQ measurement of 80. A healing
screw was then positioned (Figures 2a, b, c, d).
The patient was prescribed antibiotics and analgesics and given oral
hygiene instructions. A recall visit was scheduled after two months
for the chairside prosthetic procedure. At this visit, ISQ was re-
measured and found to be 84, confirming good secondary stability.
A postoperative radiograph confirmed proper implant positioning,
and digital impressions were taken using the CEREC workflow with a
Primescan oral scanner.
An implant scan body was used to capture impressions, and a Fig 1c: Radiographic image of the edentulous site before implant
placement.
44 Dental Practice I November-December 2024 I Vol 20 No 5