
Page 49 - DP Vol 20 No 5_Neat
P. 49
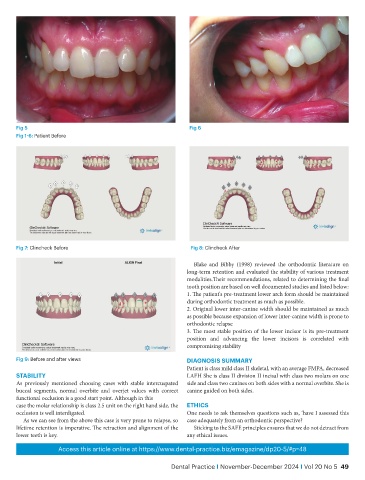
Fig 5 Fig 6
Fig 1-6: Patient Before
Fig 7: Clincheck Before Fig 8: Clincheck After
Blake and Bibby (1998) reviewed the orthodontic literature on
long-term retention and evaluated the stability of various treatment
modalities.Their recommendations, related to determining the final
tooth position are based on well documented studies and listed below:
1. The patient's pre-treatment lower arch form should be maintained
during orthodontic treatment as much as possible.
2. Original lower inter-canine width should be maintained as much
as possible because expansion of lower inter-canine width is prone to
orthodontic relapse
3. The most stable position of the lower incisor is its pre-treatment
position and advancing the lower incisors is correlated with
compromising stability
Fig 9: Before and after views DIAGNOSIS SUMMARY
Patient is class mild class II skeletal, with an average FMPA, decreased
STABILITY LAFH She is class II division II incisal with class two molars on one
As previously mentioned choosing cases with stable intercuspated side and class two canines on both sides with a normal overbite. She is
buccal segments, normal overbite and overjet values with correct canine guided on both sides.
functional occlusion is a good start point. Although in this
case the molar relationship is class 2.5 unit on the right hand side, the ETHICS
occlusion is well interdigated. One needs to ask themselves questions such as, ‘have I assessed this
As we can see from the above this case is very prone to relapse, so case adequately from an orthodontic perspective?
lifetime retention is imperative. The retraction and alignment of the Sticking to the SAFE principles ensures that we do not detract from
lower teeth is key. any ethical issues.
Access this article online at https://www.dental-practice.biz/emagazine/dp20-5/#p=48
Dental Practice I November-December 2024 I Vol 20 No 5 49