
Page 54 - DP Vol 20 No 5_Neat
P. 54
PROSTHETIC DENTISTRY SECTION
IMPLANT-PROSTHETIC REPRODUCTION OF
AN OLD TOOTH IN THE ANTERIOR REGION
THE RAVAGES OF TIME
Edwin Zanabria
Over the years, not only do we change and adapt to our environment,
but our teeth also go through similar phases. In this article, the authors
focus on the reconstruction of an old incisor that the patient had lost
and needed to be replaced with an implant-prosthesis. Useful for this
purpose were the residual adjacent teeth, which provided valuable
information. It is important to identify these relevant features and
transfer them to the restoration.
The patient was a 49-year-old man, a smoker (more than one
pack a day), with periodontal disease diagnosed three years back and
treated. He presented to the clinic due to the sudden loss of tooth
number 25. During the examination, grade III mobility of teeth
numbers 12 and 22 was also noted. To replace the missing tooth 25, an
implant was considered. Further clinical examination revealed hard
and soft calcifications and three amalgam fillings. A closer screening
and probing ruled out the presence of periodontal pockets and active
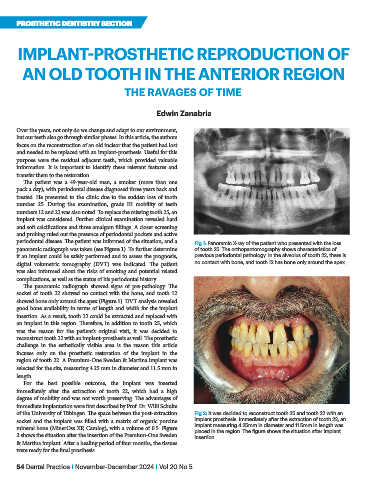
periodontal disease. The patient was informed of the situation, and a Fig 1: Panoramic X-ray of the patient who presented with the loss
panoramic radiograph was taken (see Figure 1). To further determine of tooth 25. The orthopantomography shows characteristics of
if an implant could be safely performed and to assess the prognosis, previous periodontal pathology. In the alveolus of tooth 22, there is
digital volumetric tomography (DVT) was indicated. The patient no contact with bone, and tooth 12 has bone only around the apex.
was also informed about the risks of smoking and potential related
complications, as well as the status of his periodontal history.
The panoramic radiograph showed signs of pre-pathology. The
socket of tooth 22 showed no contact with the bone, and tooth 12
showed bone only around the apex (Figure 1). DVT analysis revealed
good bone availability in terms of length and width for the implant
insertion. As a result, tooth 22 could be extracted and replaced with
an implant in this region. Therefore, in addition to tooth 25, which
was the reason for the patient’s original visit, it was decided to
reconstruct tooth 22 with an implant-prosthesis as well. The prosthetic
challenge in the esthetically visible area is the reason this article
focuses only on the prosthetic restoration of the implant in the
region of tooth 22. A Premium-One Sweden & Martina implant was
selected for the site, measuring 4.25 mm in diameter and 11.5 mm in
length.
For the best possible outcome, the implant was inserted
immediately after the extraction of tooth 22, which had a high
degree of mobility and was not worth preserving. The advantages of
immediate implantation were first described by Prof. Dr. Willi Schulte
of the University of Tübingen. The space between the post-extraction Fig 2: It was decided to reconstruct tooth 25 and tooth 22 with an
socket and the implant was filled with a matrix of organic porcine implant prosthesis. Immediately after the extraction of tooth 22, an
mineral bone (MinerOss XP, Camlog), with a volume of 0.5. Figure implant measuring 4.25mm in diameter and 11.5mm in length was
2 shows the situation after the insertion of the Premium-One Sweden placed in the region. The figure shows the situation after implant
insertion.
& Martina implant. After a healing period of four months, the tissues
were ready for the final prosthesis.
54 Dental Practice I November-December 2024 I Vol 20 No 5