
Page 236 - Feline Cardiology
P. 236
Chapter 18: Arrhythmias and Other Electrocardiographic Abnormalities 241
A B Arrhythmias
P
P P P P P P P P P
QRS
QRS QRS QRS
QRS
C
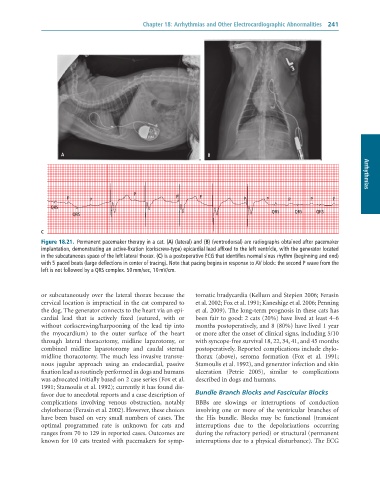
Figure 18.21. Permanent pacemaker therapy in a cat. (A) (lateral) and (B) (ventrodorsal) are radiographs obtained after pacemaker
implantation, demonstrating an active-fixation (corkscrew-type) epicardial lead affixed to the left ventricle, with the generator located
in the subcutaneous space of the left lateral thorax. (C) is a postoperative ECG that identifies normal sinus rhythm (beginning and end)
with 5 paced beats (large deflections in center of tracing). Note that pacing begins in response to AV block: the second P wave from the
left is not followed by a QRS complex. 50 mm/sec, 10 mV/cm.
or subcutaneously over the lateral thorax because the tomatic bradycardia (Kellum and Stepien 2006; Ferasin
cervical location is impractical in the cat compared to et al. 2002; Fox et al. 1991; Kaneshige et al. 2006; Penning
the dog. The generator connects to the heart via an epi- et al. 2009). The long-term prognosis in these cats has
cardial lead that is actively fixed (sutured, with or been fair to good: 2 cats (20%) have lived at least 4–6
without corkscrewing/harpooning of the lead tip into months postoperatively, and 8 (80%) have lived 1 year
the myocardium) to the outer surface of the heart or more after the onset of clinical signs, including 5/10
through lateral thoracotomy, midline laparotomy, or with syncope-free survival 18, 22, 34, 41, and 45 months
combined midline laparotoromy and caudal sternal postoperatively. Reported complications include chylo-
midline thoracotomy. The much less invasive transve- thorax (above), seroma formation (Fox et al. 1991;
nous jugular approach using an endocardial, passive Stamoulis et al. 1992), and generator infection and skin
fixation lead as routinely performed in dogs and humans ulceration (Petrie 2005), similar to complications
was advocated initially based on 2 case series (Fox et al. described in dogs and humans.
1991; Stamoulis et al. 1992); currently it has found dis-
favor due to anecdotal reports and a case description of Bundle Branch Blocks and Fascicular Blocks
complications involving venous obstruction, notably BBBs are slowings or interruptions of conduction
chylothorax (Ferasin et al. 2002). However, these choices involving one or more of the ventricular branches of
have been based on very small numbers of cases. The the His bundle. Blocks may be functional (transient
optimal programmed rate is unknown for cats and interruptions due to the depolarizations occurring
ranges from 70 to 129 in reported cases. Outcomes are during the refractory period) or structural (permanent
known for 10 cats treated with pacemakers for symp- interruptions due to a physical disturbance). The ECG