
Page 233 - Feline Cardiology
P. 233
238 Section F: Arrhythmias and Other Electrocardiographic Abnormalities
in the AV node and is said to carry a good prognosis undertaken using an atropine response test: an ECG
because it is closely related to first-degree AV block and strip is recorded, and 0.04 mg/kg atropine is immedi-
virtually never causes clinical signs. This form of second- ately administered IV. One or both follow-up ECGs
degree AV block is very uncommon in the cat, perhaps recorded 15 and 30 minutes later should show sinus
because, like first-degree AV block, it usually arises in tachycardia when second-degree AV block is vagally
states of parasympathetic predominance. The other type mediated and therefore likely harmless; this is more
of second-degree AV block, Mobitz type II, by contrast likely with Mobitz type I than II, but either type may
demonstrates perfectly regular PR intervals for all QRS respond to atropine. If atropine response is noted, and
complexes, until suddenly one or more P wave(s) is/are the cat displayed symptoms consistent with poor arterial
blocked. Mobitz type II second-degree AV block arises perfusion, such as syncope, treatment with terbutaline
from the AV bundle and is said to carry a more guarded may be tried (0.625 mg PO q 8–12h); propantheline
to poor prognosis because it more closely resembles (0.8–1.6 mg/kg PO q 8h, titrate down or stop if constipa-
third-degree AV block. However, objective evidence is tion or other extracardiac vagolytic signs occur) is a
lacking to support this extrapolation of severity in second choice if terbutaline is not effective or not toler-
Mobitz types I and II from human cardiology to feline ated. However, many syncopal cats with AV block ulti-
patients. In “simple” Mobitz type II second-degree AV mately may require a pacemaker (see below). In the
Arrhythmias waves, whereas in “advanced” or “high grade” Mobitz syncope, treatment of second-degree AV block generally
absence of overt clinical signs such as weakness or
block, more conducted P waves occur than blocked P
is not necessary. An exception to this rule is a stable
type II second-degree AV block (Figure 18.19), more
blocked P waves occur than conducted P waves. The
presence or absence of clinical signs in second-degree patient that requires general anesthesia, where bradycar-
dia that is unresponsive to anticholinergics may develop
AV block appears to be related to the overall ventricular intraoperatively. Cats with high-grade second-degree AV
rate. Therefore Mobitz type I second-degree AV block block should be instrumented with a temporary pace-
essentially never produces clinical manifestations such maker (Côté and Laste 2000; Petrie 2005) if they require
as lethargy or syncope, whereas the more advanced general anesthesia, as they may otherwise arrest or
Mobitz type II second-degree AV block cases often have develop severe bradycardia at induction or during main-
clinical signs that are similar to third-degree AV block, tenance, and drugs that only accelerate SA nodal activity
concurrent with a slow ventricular rate (100 beats/ (atropine, glycopyrrolate, epinephrine) are likely to be
minute or less): weakness, lethargy, syncope, and cardio- ineffective because they rarely increase conduction
genic seizures (true convulsions caused by critical, speed through a diseased AV node. In second-degree AV
bradycardia-induced cerebral hypoperfusion) even with block, drugs with negative chronotropic properties,
minimal exertion. including beta blockers and calcium-channel blockers,
Assessment of the physiologic (generally harmless) are contraindicated.
versus pathologic (may cause clinical signs such as Third-degree AV block is a complete and sustained
syncope) nature of second-degree AV block may be interruption of AV conduction. The only ventricular
* * *
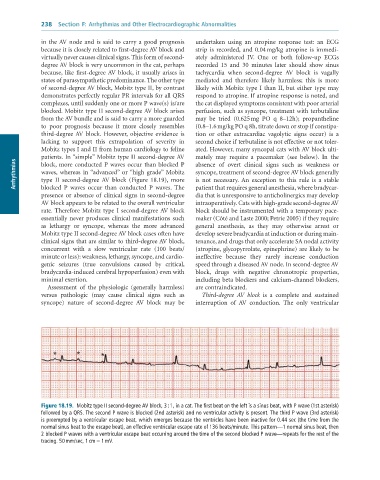
Figure 18.19. Mobitz type II second-degree AV block, 3 : 1, in a cat. The first beat on the left is a sinus beat, with P wave (1st asterisk)
followed by a QRS. The second P wave is blocked (2nd asterisk) and no ventricular activity is present. The third P wave (3rd asterisk)
is preempted by a ventricular escape beat, which emerges because the ventricles have been inactive for 0.44 sec (the time from the
normal sinus beat to the escape beat), an effective ventricular escape rate of 136 beats/minute. This pattern—1 normal sinus beat, then
2 blocked P waves with a ventricular escape beat occurring around the time of the second blocked P wave—repeats for the rest of the
tracing. 50 mm/sec, 1 cm = 1 mV.