
Page 433 - Withrow and MacEwen's Small Animal Clinical Oncology, 6th Edition
P. 433
CHAPTER 22 Soft Tissue Sarcomas 411
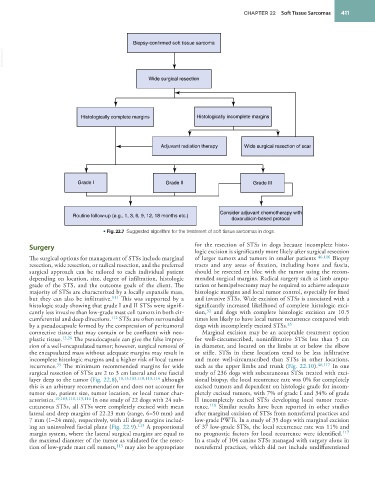
Biopsy-confirmed soft tissue sarcoma
VetBooks.ir
Wide surgical resection
Histologically complete margins Histologically incomplete margins
Adjuvant radiation therapy Wide surgical resection of scar
Grade I Grade II Grade III
Consider adjuvant chemotherapy with
Routine follow-up (e.g., 1, 3, 6, 9, 12, 18 months etc.)
doxorubicin-based protocol
• Fig. 22.7 Suggested algorithm for the treatment of soft tissue sarcomas in dogs.
Surgery for the resection of STSs in dogs because incomplete histo-
logic excision is significantly more likely after surgical resection
The surgical options for management of STSs include marginal of larger tumors and tumors in smaller patients 46,116 Biopsy
resection, wide resection, or radical resection, and the preferred tracts and any areas of fixation, including bone and fascia,
surgical approach can be tailored to each individual patient should be resected en bloc with the tumor using the recom-
depending on location, size, degree of infiltration, histologic mended surgical margins. Radical surgery such as limb ampu-
grade of the STS, and the outcome goals of the client. The tation or hemipelvectomy may be required to achieve adequate
majority of STSs are characterized by a locally expansile mass, histologic margins and local tumor control, especially for fixed
but they can also be infiltrative. 111 This was supported by a and invasive STSs. Wide excision of STSs is associated with a
histologic study showing that grade I and II STSs were signifi- significantly increased likelihood of complete histologic exci-
cantly less invasive than low-grade mast cell tumors in both cir- sion, and dogs with complete histologic excision are 10.5
32
cumferential and deep directions. 112 STSs are often surrounded times less likely to have local tumor recurrence compared with
by a pseudocapsule formed by the compression of peritumoral dogs with incompletely excised STSs. 35
connective tissue that may contain or be confluent with neo- Marginal excision may be an acceptable treatment option
plastic tissue. 12,26 The pseudocapsule can give the false impres- for well-circumscribed, noninfiltrative STSs less than 5 cm
sion of a well-encapsulated tumor; however, surgical removal of in diameter, and located on the limbs at or below the elbow
the encapsulated mass without adequate margins may result in or stifle. STSs in these locations tend to be less infiltrative
incomplete histologic margins and a higher risk of local tumor and more well-circumscribed than STSs in other locations,
35
recurrence. The minimum recommended margins for wide such as the upper limbs and trunk (Fig. 22.10). 46,117 In one
surgical resection of STSs are 2 to 3 cm lateral and one fascial study of 236 dogs with subcutaneous STSs treated with exci-
layer deep to the tumor (Fig. 22.8), 10,13,103,110,113,114 although sional biopsy, the local recurrence rate was 0% for completely
this is an arbitrary recommendation and does not account for excised tumors and dependent on histologic grade for incom-
tumor size, patient size, tumor location, or local tumor char- pletely excised tumors, with 7% of grade I and 34% of grade
acteristics. 10,103,110,113,114 In one study of 22 dogs with 24 sub- II incompletely excised STSs developing local tumor recur-
cutaneous STSs, all STSs were completely excised with mean rence. 118 Similar results have been reported in other studies
lateral and deep margins of 22.23 mm (range, 6–50 mm) and after marginal excision of STSs from nonreferral practices and
7 mm (1–24 mm), respectively, with all deep margins includ- low-grade PWTs. In a study of 35 dogs with marginal excision
ing an uninvolved fascial plane (Fig. 22.9). 113 A proportional of 37 low-grade STSs, the local recurrence rate was 11% and
margin system, where the lateral surgical margins are equal to no prognostic factors for local recurrence were identified. 117
the maximal diameter of the tumor as validated for the resec- In a study of 104 canine STSs managed with surgery alone in
tion of low-grade mast cell tumors, 115 may also be appropriate nonreferral practices, which did not include undifferentiated