
Page 23 - GP Spring 2020
P. 23
Abfraction, Abrasion, Attrition and Erosion
By Gwen Cohen Brown, DDS, FAAOMP and Maria Elena Bilello, RDH, MSPH
Dentistry is not “black and white.” There Most patients are older although the exact is using a hard bristled toothbrush using a
are many situations that cause our patients age is not consistent in the literature. Race back and forth motion. (Figures 4,5)
to leave unsatisfied, unclear why the ‘prob- is inconsequential.
lem’ cannot be fixed. Even less clear to
them is how they caused situations that Treatment: It is important to remember
are now irreversible and may require costly when treating abfractions that the dentist is
solutions. not treating the etiology of the disease pro-
cess, only the clinical manifestations of that
On a daily basis dental professionals at- process. They are replacing the tooth that
tempt to explain attrition, abrasion, erosion has been lost. Most clinicians replace with
and abfraction to our patients with variable composite fillings or glass ionomer fillings
degrees of efficacy. It is important to re- initially. If the lesions recur, or the resto-
fresh the importance of these conditions as rations cannot be maintained, then a full
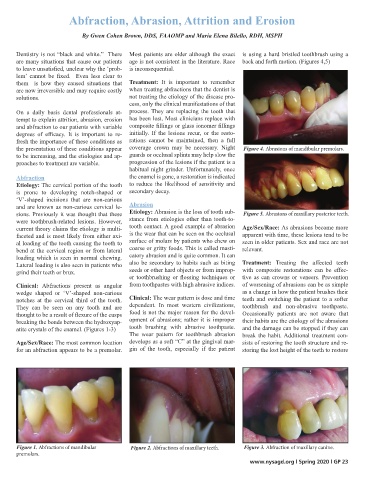
the presentation of these conditions appear coverage crown may be necessary. Night Figure 4. Abrasions of mandibular premolars.
to be increasing, and the etiologies and ap- guards or occlusal splints may help slow the
proaches to treatment are variable. progression of the lesions if the patient is a
habitual night grinder. Unfortunately, once
Abfraction the enamel is gone, a restoration is indicated
Etiology: The cervical portion of the tooth to reduce the likelihood of sensitivity and
is prone to developing notch-shaped or secondary decay.
‘V’-shaped incisions that are non-carious
and are known as non-carious cervical le- Abrasion
sions. Previously it was thought that these Etiology: Abrasion is the loss of tooth sub- Figure 5. Abrasions of maxillary posterior teeth.
were toothbrush-related lesions. However, stance from etiologies other than tooth-to-
current theory claims the etiology is multi- tooth contact. A good example of abrasion Age/Sex/Race: As abrasions become more
faceted and is most likely from either axi- is the wear that can be seen on the occlusal apparent with time, these lesions tend to be
al loading of the tooth causing the tooth to surface of molars by patients who chew on seen in older patients. Sex and race are not
bend at the cervical region or from lateral coarse or gritty foods. This is called masti- relevant.
loading which is seen in normal chewing. catory abrasion and is quite common. It can
Lateral loading is also seen in patients who also be secondary to habits such as biting Treatment: Treating the affected teeth
grind their teeth or brux. seeds or other hard objects or from improp- with composite restorations can be effec-
er toothbrushing or flossing techniques or tive as can crowns or veneers. Prevention
Clinical: Abfractions present as angular from toothpastes with high abrasive indices. of worsening of abrasions can be as simple
wedge shaped or ‘V’-shaped non-carious as a change in how the patient brushes their
notches at the cervical third of the tooth. Clinical: The wear pattern is dose and time teeth and switching the patient to a softer
They can be seen on any tooth and are dependent. In most western civilizations, toothbrush and non-abrasive toothpaste.
thought to be a result of flexure of the cusps food is not the major reason for the devel- Occasionally patients are not aware that
breaking the bonds between the hydroxyap- opment of abrasions; rather it is improper their habits are the etiology of the abrasions
atite crystals of the enamel. (Figures 1-3) tooth brushing with abrasive toothpaste. and the damage can be stopped if they can
The wear pattern for toothbrush abrasion break the habit. Additional treatment con-
Age/Sex/Race: The most common location develops as a soft “C” at the gingival mar- sists of restoring the tooth structure and re-
for an abfraction appears to be a premolar. gin of the tooth, especially if the patient storing the lost height of the teeth to restore
Figure 1. Abfractions of mandibular Figure 2. Abfractions of maxillary teeth. Figure 3. Abfraction of maxillary canine.
premolars.
www.nysagd.org l Spring 2020 l GP 23