
Page 11 - Walter Robbs 2018 Benefit Guide
P. 11
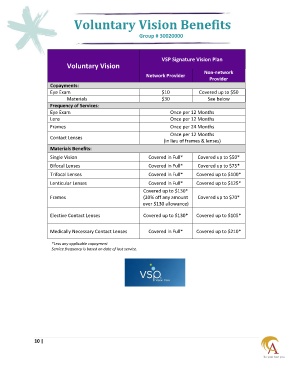
Voluntary Vision Benefits
Group # 30020000
VSP Signature Vision Plan
Voluntary Vision
Network Provider Non-network
Provider
Copayments:
Eye Exam $10 Covered up to $50
Materials $30 See below
Frequency of Services:
Eye Exam Once per 12 Months
Lens Once per 12 Months
Frames Once per 24 Months
Once per 12 Months
Contact Lenses
(in lieu of frames & lenses)
Materials Benefits:
Single Vision Covered in Full* Covered up to $50*
Bifocal Lenses Covered in Full* Covered up to $75*
Trifocal Lenses Covered in Full* Covered up to $100*
Lenticular Lenses Covered in Full* Covered up to $125*
Covered up to $130*
Frames (20% off any amount Covered up to $70*
over $130 allowance)
Elective Contact Lenses Covered up to $130* Covered up to $105*
Medically Necessary Contact Lenses Covered in Full* Covered up to $210*
*Less any applicable copayment
Service frequency is based on date of last service.
10 |