
Page 10 - RS&A Benefits Enrollments Guide
P. 10
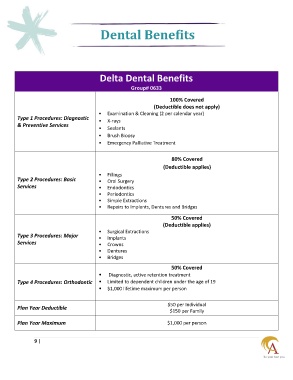
Dental Benefits
Delta Dental Benefits
Group# 0633
100% Covered
(Deductible does not apply)
• Examination & Cleaning (2 per calendar year)
Type 1 Procedures: Diagnostic
• X-rays
& Preventive Services
• Sealants
• Brush Biopsy
• Emergency Palliative Treatment
80% Covered
(Deductible applies)
• Fillings
Type 2 Procedures: Basic • Oral Surgery
Services • Endodontics
• Periodontics
• Simple Extractions
• Repairs to Implants, Dentures and Bridges
50% Covered
(Deductible applies)
• Surgical Extractions
Type 3 Procedures: Major • Implants
Services • Crowns
• Dentures
• Bridges
50% Covered
• Diagnostic, active retention treatment
Type 4 Procedures: Orthodontic • Limited to dependent children under the age of 19
• $1,000 lifetime maximum per person
$50 per Individual
Plan Year Deductible
$150 per Family
Plan Year Maximum $1,000 per person
9 |