
Page 100 - Medicine and Surgery
P. 100
P1: FAW
BLUK007-03 BLUK007-Kendall May 25, 2005 17:29 Char Count= 0
96 Chapter 3: Respiratory system
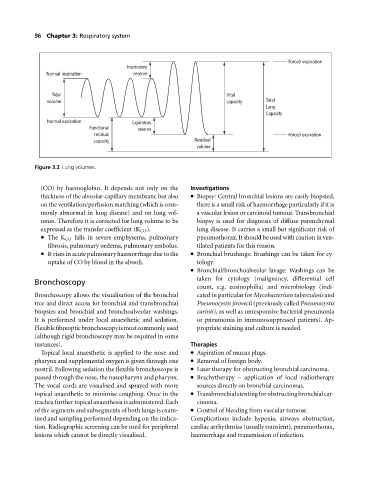
Forced inspiration
Inspiratory
Normal inspiration reserve
Tidal Vital
volume capacity Total
Lung
Capacity
Normal expiration Expiratory
Functional reserve
residual Forced expiration
capacity Residual
volume
Figure 3.2 Lung volumes.
(CO) by haemoglobin. It depends not only on the Investigations
thickness of the alveolar-capillary membrane but also Biopsy: Central bronchial lesions are easily biopsied,
on the ventilation/perfusion matching (which is com- there is a small risk of haemorrhage particularly if it is
monly abnormal in lung disease) and on lung vol- avascular lesion or carcinoid tumour. Transbronchial
umes. Therefore it is corrected for lung volume to be biopsy is used for diagnosis of diffuse parenchymal
expressed as the transfer coefficient (K CO ). lung disease. It carries a small but significant risk of
The K CO falls in severe emphysema, pulmonary pneumothorax. It should be used with caution in ven-
fibrosis, pulmonary oedema, pulmonary embolus. tilated patients for this reason.
It rises in acute pulmonary haemorrhage due to the Bronchial brushings: Brushings can be taken for cy-
uptake of CO by blood in the alveoli. tology.
Bronchial/bronchoalveolar lavage: Washings can be
taken for cytology (malignancy, differential cell
Bronchoscopy
count, e.g. eosinophilia) and microbiology (indi-
Bronchoscopy allows the visualisation of the bronchial cated in particular for Mycobacterium tuberculosis and
tree and direct access for bronchial and transbronchial Pneumocystis jirovecii (previously called Pneumocystis
biopsies and bronchial and bronchoalveolar washings. carinii),aswellasunresponsive bacterial pneumonia
It is performed under local anaesthetic and sedation. or pneumonia in immunosuppressed patients). Ap-
Flexiblefibreopticbronchoscopyismostcommonlyused propriate staining and culture is needed.
(although rigid bronchoscopy may be required in some
instances). Therapies
Topical local anaesthetic is applied to the nose and Aspiration of mucus plugs.
pharynx and supplemental oxygen is given through one Removal of foreign body.
nostril. Following sedation the flexible bronchoscope is Laser therapy for obstructing bronchial carcinoma.
passed through the nose, the nasopharynx and pharynx. Brachytherapy – application of local radiotherapy
The vocal cords are visualised and sprayed with more sources directly on bronchial carcinomas.
topical anaesthetic to minimise coughing. Once in the Transbronchialstentingforobstructingbronchialcar-
trachea further topical anaesthesia is administered. Each cinoma.
of the segments and subsegments of both lungs is exam- Control of bleeding from vascular tumour.
ined and sampling performed depending on the indica- Complications include hypoxia, airways obstruction,
tion. Radiographic screening can be used for peripheral cardiac arrhythmias (usually transient), pneumothorax,
lesions which cannot be directly visualised. haemorrhage and transmission of infection.