
Page 13 - NYMets_2018_Benefits_Guide
P. 13
BACK TO
HOME
PLATE
at-bat: medical benefits
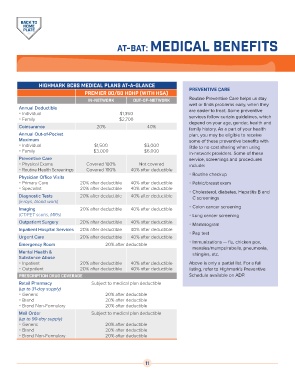
Highmark bcbs medical plans at-a-glance
preventive care
Premier 80/60 HDHP (with HSA)
in-network out-of-network Routine Preventive Care helps us stay
well or finds problems early, when they
Annual Deductible are easier to treat. Some preventive
Individual $1,350
Family $2,700 services follow certain guidelines, which
depend on your age, gender, health and
Coinsurance 20% 40%
family history. As a part of your health
Annual Out-of-Pocket plan, you may be eligible to receive
Maximum some of these preventive benefits with
Individual $1,500 $3,000 little to no cost sharing when using
Family $3,000 $6,000
in-network providers. Some of these
Preventive Care service, screenings and procedures
Physical Exams Covered 100% Not covered include:
Routine Health Screenings Covered 100% 40% after deductible
Routine checkup
Physician Office Visits
Primary Care 20% after deductible 40% after deductible Pelvic/breast exam
Specialist 20% after deductible 40% after deductible
Cholesterol, diabetes, Hepatitis B and
Diagnostic Tests 20% after deductible 40% after deductible C screenings
(x-rays, blood work)
Imaging 20% after deductible 40% after deductible Colon cancer screening
(CT/PET scans, MRIs) Lung cancer screening
Outpatient Surgery 20% after deductible 40% after deductible Mammogram
Inpatient Hospital Services 20% after deductible 40% after deductible
Pap test
Urgent Care 20% after deductible 40% after deductible
Immunizations — flu, chicken pox,
Emergency Room 20% after deductible
measles/mumps/rubella, pneumonia,
Mental Health & shingles, etc.
Substance Abuse
Inpatient 20% after deductible 40% after deductible Above is only a partial list. For a full
Outpatient 20% after deductible 40% after deductible listing, refer to Highmark’s Preventive
Prescription Drug Coverage Schedule available on ADP.
Retail Pharmacy Subject to medical plan deductible
(up to 31-day supply)
Generic 20% after deductible
Brand 20% after deductible
Brand Non-Formulary 20% after deductible
Mail Order Subject to medical plan deductible
(up to 90-day supply)
Generic 20% after deductible
Brand 20% after deductible
Brand Non-Formulary 20% after deductible
11