
Page 197 - Zoo Animal Learning and Training
P. 197
Chapter 23: Thoracolumbar Lateral Corpectomy 201
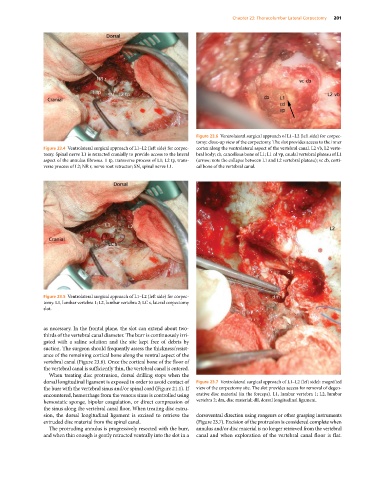
Figure 23.6 Ventrolateral surgical approach of L1–L2 (left side) for corpec-
tomy: close‐up view of the corpectomy. The slot provides access to the inner
Figure 23.4 Ventrolateral surgical approach of L1–L2 (left side) for corpec- cortex along the ventrolateral aspect of the vertebral canal. L2 vb, L2 verte-
tomy. Spinal nerve L1 is retracted cranially to provide access to the lateral bral body; cb, cancellous bone of L1; L1 cd vp, caudal vertebral plateau of L1
aspect of the annulus fibrosus. 1 tp, transverse process of L1; L2 tp, trans- (arrow; note the collapse between L1 and L2 vertebral plateau); vc cb, corti-
verse process of L2; NR r, nerve root retractor; SN, spinal nerve L1. cal bone of the vertebral canal.
Figure 23.5 Ventrolateral surgical approach of L1–L2 (left side) for corpec-
tomy. L1, lumbar vertebra 1; L2, lumbar vertebra 2; LC s, lateral corpectomy
slot.
as necessary. In the frontal plane, the slot can extend about two‐
thirds of the vertebral canal diameter. The burr is continuously irri-
gated with a saline solution and the site kept free of debris by
suction. The surgeon should frequently assess the thickness/resist-
ance of the remaining cortical bone along the ventral aspect of the
vertebral canal (Figure 23.6). Once the cortical bone of the floor of
the vertebral canal is sufficiently thin, the vertebral canal is entered.
When treating disc protrusion, dorsal drilling stops when the
dorsal longitudinal ligament is exposed in order to avoid contact of Figure 23.7 Ventrolateral surgical approach of L1–L2 (left side): magnified
the burr with the vertebral sinus and/or spinal cord (Figure 21.1). If view of the corpectomy site. The slot provides access for removal of degen-
encountered, hemorrhage from the venous sinus is controlled using erative disc material (in the forceps). L1, lumbar vertebra 1; L2, lumbar
hemostatic sponge, bipolar coagulation, or direct compression of vertebra 2; dm, disc material; dll, dorsal longitudinal ligament.
the sinus along the vertebral canal floor. When treating disc extru-
sion, the dorsal longitudinal ligament is excised to retrieve the dorsoventral direction using rongeurs or other grasping instruments
extruded disc material from the spinal canal. (Figure 23.7). Excision of the protrusion is considered complete when
The protruding annulus is progressively resected with the burr, annulus and/or disc material is no longer retrieved from the vertebral
and when thin enough is gently retracted ventrally into the slot in a canal and when exploration of the vertebral canal floor is flat.