
Page 1068 - Small Animal Internal Medicine, 6th Edition
P. 1068
1040 PART IX Nervous System and Neuromuscular Disorders
produce contraction (see Fig. 58.2). Damage to any compo- information from the higher centers to the LMN. These
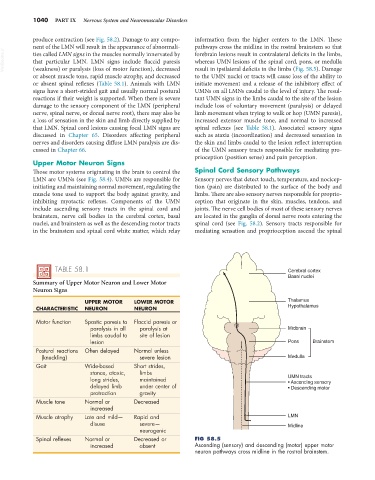
nent of the LMN will result in the appearance of abnormali- pathways cross the midline in the rostral brainstem so that
VetBooks.ir ties called LMN signs in the muscles normally innervated by forebrain lesions result in contralateral deficits in the limbs,
whereas UMN lesions of the spinal cord, pons, or medulla
that particular LMN. LMN signs include flaccid paresis
(weakness) or paralysis (loss of motor function), decreased
to the UMN nuclei or tracts will cause loss of the ability to
or absent muscle tone, rapid muscle atrophy, and decreased result in ipsilateral deficits in the limbs (Fig. 58.5). Damage
or absent spinal reflexes (Table 58.1). Animals with LMN initiate movement and a release of the inhibitory effect of
signs have a short-strided gait and usually normal postural UMNs on all LMNs caudal to the level of injury. The resul-
reactions if their weight is supported. When there is severe tant UMN signs in the limbs caudal to the site of the lesion
damage to the sensory component of the LMN (peripheral include loss of voluntary movement (paralysis) or delayed
nerve, spinal nerve, or dorsal nerve root), there may also be limb movement when trying to walk or hop (UMN paresis),
a loss of sensation in the skin and limb directly supplied by increased extensor muscle tone, and normal to increased
that LMN. Spinal cord lesions causing focal LMN signs are spinal reflexes (see Table 58.1). Associated sensory signs
discussed in Chapter 65. Disorders affecting peripheral such as ataxia (incoordination) and decreased sensation in
nerves and disorders causing diffuse LMN paralysis are dis- the skin and limbs caudal to the lesion reflect interruption
cussed in Chapter 66. of the UMN sensory tracts responsible for mediating pro-
prioception (position sense) and pain perception.
Upper Motor Neuron Signs
Those motor systems originating in the brain to control the Spinal Cord Sensory Pathways
LMN are UMNs (see Fig. 58.4). UMNs are responsible for Sensory nerves that detect touch, temperature, and nocicep-
initiating and maintaining normal movement, regulating the tion (pain) are distributed to the surface of the body and
muscle tone used to support the body against gravity, and limbs. There are also sensory nerves responsible for proprio-
inhibiting myotactic reflexes. Components of the UMN ception that originate in the skin, muscles, tendons, and
include ascending sensory tracts in the spinal cord and joints. The nerve cell bodies of most of these sensory nerves
brainstem, nerve cell bodies in the cerebral cortex, basal are located in the ganglia of dorsal nerve roots entering the
nuclei, and brainstem as well as the descending motor tracts spinal cord (see Fig. 58.2). Sensory tracts responsible for
in the brainstem and spinal cord white matter, which relay mediating sensation and proprioception ascend the spinal
TABLE 58.1 Cerebral cortex
Basal nuclei
Summary of Upper Motor Neuron and Lower Motor
Neuron Signs
UPPER MOTOR LOWER MOTOR Thalamus
CHARACTERISTIC NEURON NEURON Hypothalamus
Motor function Spastic paresis to Flaccid paresis or
paralysis in all paralysis at Midbrain
limbs caudal to site of lesion
lesion Pons Brainstem
Postural reactions Often delayed Normal unless
(knuckling) severe lesion Medulla
Gait Wide-based Short strides,
stance, ataxic, limbs
long strides, maintained UMN tracts
• Ascending sensory
delayed limb under center of • Descending motor
protraction gravity
Muscle tone Normal or Decreased
increased
Muscle atrophy Late and mild— Rapid and LMN
disuse severe— Midline
neurogenic
Spinal reflexes Normal or Decreased or FIG 58.5
increased absent Ascending (sensory) and descending (motor) upper motor
neuron pathways cross midline in the rostral brainstem.