
Page 450 - Small Animal Clinical Nutrition 5th Edition
P. 450
464 Small Animal Clinical Nutrition
VetBooks.ir Box 25-8. Surgical Gastrostomy Tube Placement.
A limited left flank celiotomy for gastrostomy tube placement
provides an alternative when endoscopic or blind gastrostomy
techniques are not performed. A gastrostomy tube may also be
inserted when a celiotomy is performed for other reasons.
General anesthesia is administered and the left flank is asepti-
cally prepared for surgery. The prepared left paracostal area is
draped and a 2- to 3-cm incision is made through the skin and
subcutaneous tissue. The incision is made just caudal and par-
allel to the last rib, with its dorsal limit just below the ventral
edge of the paravertebral epaxial musculature. The incision
should be extended ventrally so that the intraperitoneal rather
than the retroperitoneal space is accessed. The incision should
be long enough to permit insertion of one or two fingers and a
tissue forceps.
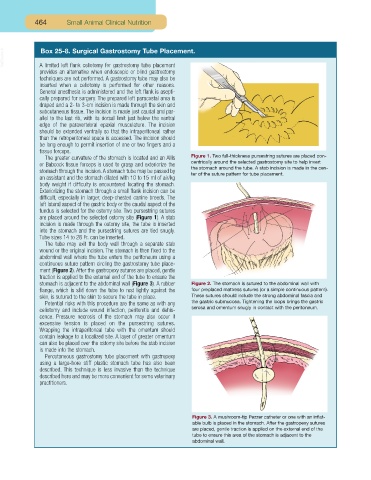
The greater curvature of the stomach is located and an Allis Figure 1. Two full-thickness pursestring sutures are placed con-
or Babcock tissue forceps is used to grasp and exteriorize the centrically around the selected gastrostomy site to help invert
stomach through the incision.A stomach tube may be passed by the stomach around the tube. A stab incision is made in the cen-
ter of the suture pattern for tube placement.
an assistant and the stomach dilated with 10 to 15 ml of air/kg
body weight if difficulty is encountered locating the stomach.
Exteriorizing the stomach through a small flank incision can be
difficult, especially in larger, deep-chested canine breeds. The
left lateral aspect of the gastric body or the caudal aspect of the
fundus is selected for the ostomy site. Two pursestring sutures
are placed around the selected ostomy site (Figure 1). A stab
incision is made through the ostomy site, the tube is inserted
into the stomach and the pursestring sutures are tied snugly.
Tube sizes 14 to 28 Fr. can be inserted.
The tube may exit the body wall through a separate stab
wound or the original incision. The stomach is then fixed to the
abdominal wall where the tube enters the peritoneum using a
continuous suture pattern circling the gastrostomy tube place-
ment (Figure 2). After the gastropexy sutures are placed, gentle
traction is applied to the external end of the tube to ensure the
stomach is adjacent to the abdominal wall (Figure 3). A rubber Figure 2. The stomach is sutured to the abdominal wall with
flange, which is slid down the tube to rest lightly against the four preplaced mattress sutures (or a simple continuous pattern).
skin, is sutured to the skin to secure the tube in place. These sutures should include the strong abdominal fascia and
Potential risks with this procedure are the same as with any the gastric submucosa. Tightening the loops brings the gastric
celiotomy and include wound infection, peritonitis and dehis- serosa and omentum snugly in contact with the peritoneum.
cence. Pressure necrosis of the stomach may also occur if
excessive tension is placed on the pursestring sutures.
Wrapping the intraperitoneal tube with the omentum should
contain leakage to a localized site. A layer of greater omentum
can also be placed over the ostomy site before the stab incision
is made into the stomach.
Percutaneous gastrostomy tube placement with gastropexy
using a large-bore stiff plastic stomach tube has also been
described. This technique is less invasive than the technique
described here and may be more convenient for some veterinary
practitioners.
Figure 3. A mushroom-tip Pezzer catheter or one with an inflat-
able bulb is placed in the stomach. After the gastropexy sutures
are placed, gentle traction is applied on the external end of the
tube to ensure this area of the stomach is adjacent to the
abdominal wall.