
Page 10 - Burnham EE Guide 01-20
P. 10
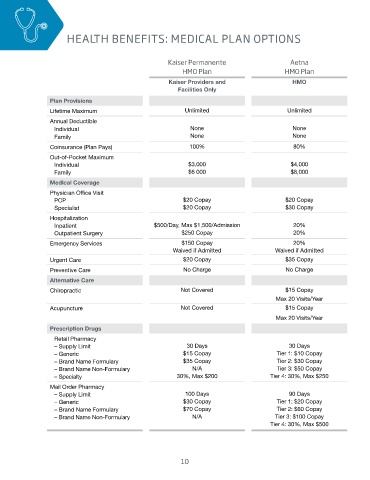
HEALTH BENEFITS: MEDICAL PLAN OPTIONS
Kaiser Permanente Aetna
HMO Plan HMO Plan
Kaiser Providers and HMO
Facilities Only
Plan Provisions
Lifetime Maximum Unlimited Unlimited
Annual Deductible
Individual None None
Family None None
Coinsurance (Plan Pays) 100% 80%
Out-of-Pocket Maximum
Individual $3,000 $4,000
Family $6 000 $8,000
Medical Coverage
Physician Office Visit
PCP $20 Copay $20 Copay
Specialist $20 Copay $30 Copay
Hospitalization
Inpatient $500/Day, Max $1,500/Admission 20%
Outpatient Surgery $250 Copay 20%
Emergency Services $150 Copay 20%
Waived if Admitted Waived if Admitted
Urgent Care $20 Copay $35 Copay
Preventive Care No Charge No Charge
Alternative Care
Chiropractic Not Covered $15 Copay
Max 20 Visits/Year
Acupuncture Not Covered $15 Copay
Max 20 Visits/Year
Prescription Drugs
Retail Pharmacy
– Supply Limit 30 Days 30 Days
– Generic $15 Copay Tier 1: $10 Copay
– Brand Name Formulary $35 Copay Tier 2: $30 Copay
– Brand Name Non-Formulary N/A Tier 3: $50 Copay
– Specialty 30%, Max $200 Tier 4: 30%, Max $250
Mail Order Pharmacy
– Supply Limit 100 Days 90 Days
– Generic $30 Copay Tier 1: $20 Copay
– Brand Name Formulary $70 Copay Tier 2: $60 Copay
– Brand Name Non-Formulary N/A Tier 3: $100 Copay
Tier 4: 30%, Max $500
10