
Page 63 - Children Bookt.pdf
P. 63
15. HIV and Nutrition
HIV-infected children should be routinely assessed for nutritional status, including
weight and height at scheduled visits, particularly after initiation of ART.
HIV-infected children on or off ART who are symptomatic, have conditions requiring
increased energy (e.g. TB, chronic lung disease, chronic OIs or malignancies), or
have weight loss or evidence of poor growth should be provided with 25 – 30%
additional energy.
HIV-infected children who are severely malnourished should be managed as per the
guidelines for uninfected children and provided with 50 – 100% additional energy.
HIV-infected children should receive one recommended daily allowance (RDA) of
micronutrients daily. If this cannot be assured through the diet, or there is evidence
'
$
!6
'
_{
$
6
$
$
_
uninfected children.
HIV-infected children who have diarrhoea should receive zinc supplementation as
part of management, as per the guidelines for uninfected children.
For infants and young children known to be HIV infected, mothers are strongly
&$
'
_
'
recommendations for the general population (up to two years of age and beyond).
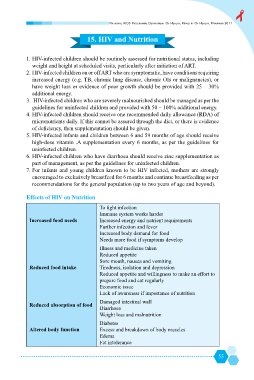
Effects of HIV on Nutrition
Immune system works harder
Increased food needs Increased energy and nutrient requirements
Further infection and fever
Increased body demand for food
Needs more food if symptoms develop
Illness and medicine taken
Reduced appetite
Sore mouth, nausea and vomiting
Reduced food intake Tiredness, isolation and depression
Reduced appetite and willingness to make an effort to
prepare food and eat regularly
Economic issue
Lack of awareness if importance of nutrition
Damaged intestinal wall
Reduced absorption of food
Diarrhoea
Weight loss and malnutrition
Diabetes
Altered body function Z&
'
'
Edema
Fat intolerance
55