
Page 8 - TriStar Energy-2023-Benefit Guide-V26(WLP)-LRI
P. 8
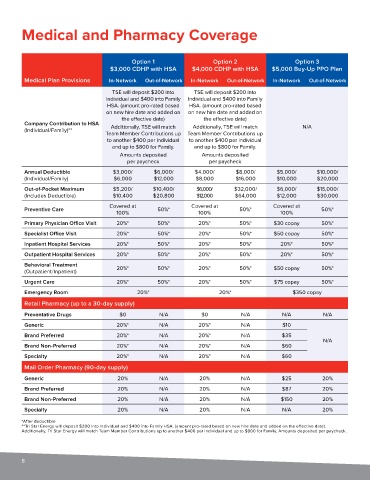
Medical and Pharmacy Coverage
Option 1 Option 2 Option 3
$3,000 CDHP with HSA $4,000 CDHP with HSA $5,000 Buy-Up PPO Plan
Medical Plan Provisions In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
TSE will deposit $200 into TSE will deposit $200 into
Individual and $400 into Family Individual and $400 into Family
HSA. (amount pro-rated based HSA. (amount pro-rated based
on new hire date and added on on new hire date and added on
the effective date) the effective date)
Company Contribution to HSA Additionally, TSE will match Additionally, TSE will match N/A
(Individual/Family)**
Team Member Contributions up Team Member Contributions up
to another $400 per individual to another $400 per individual
and up to $800 for Family. and up to $800 for Family.
Amounts deposited Amounts deposited
per paycheck per paycheck
Annual Deductible $3,000/ $6,000/ $4,000/ $8,000/ $5,000/ $10,000/
(Individual/Family) $6,000 $12,000 $8,000 $16,000 $10,000 $20,000
Out-of-Pocket Maximum $5,200/ $10,400/ $6,000/ $32,000/ $6,000/ $15,000/
(Includes Deductible) $10,400 $20,800 $12,000 $64,000 $12,000 $30,000
Covered at Covered at Covered at
Preventive Care 50%* 50%* 50%*
100% 100% 100%
Primary Physician Office Visit 20%* 50%* 20%* 50%* $30 copay 50%*
Specialist Office Visit 20%* 50%* 20%* 50%* $50 copay 50%*
Inpatient Hospital Services 20%* 50%* 20%* 50%* 20%* 50%*
Outpatient Hospital Services 20%* 50%* 20%* 50%* 20%* 50%*
Behavioral Treatment 20%* 50%* 20%* 50%* $50 copay 50%*
(Outpatient/Inpatient)
Urgent Care 20%* 50%* 20%* 50%* $75 copay 50%*
Emergency Room 20%* 20%* $350 copay
Retail Pharmacy (up to a 30-day supply)
Preventative Drugs $0 N/A $0 N/A N/A N/A
Generic 20%* N/A 20%* N/A $10
Brand Preferred 20%* N/A 20%* N/A $35
N/A
Brand Non-Preferred 20%* N/A 20%* N/A $60
Specialty 20%* N/A 20%* N/A $60
Mail Order Pharmacy (90-day supply)
Generic 20% N/A 20% N/A $25 20%
Brand Preferred 20% N/A 20% N/A $87 20%
Brand Non-Preferred 20% N/A 20% N/A $150 20%
Specialty 20% N/A 20% N/A N/A 20%
*After deductible
**Tri Star Energy will deposit $200 into Individual and $400 into Family HSA. (amount pro-rated based on new hire date and added on the effective date).
Additionally, Tri Star Energy will match Team Member Contributions up to another $400 per individual and up to $800 for Family. Amounts deposited per paycheck.
8