
Page 69 - Diamicron MR MIG Cycle 2(20-21) Final
P. 69
2424 ZACCARDI ET AL.
(A) (B)
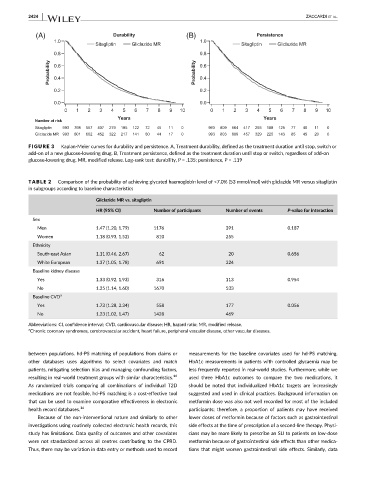
FIGURE 3 Kaplan-Meier curves for durability and persistence. A, Treatment durability, defined as the treatment duration until stop, switch or
add-on of a new glucose-lowering drug. B, Treatment persistence, defined as the treatment duration until stop or switch, regardless of add-on
glucose-lowering drug. MR, modified release. Log-rank test: durability, P = .135; persistence, P = .119
TABLE 2 Comparison of the probability of achieving glycated haemoglobin level of <7.0% (53 mmol/mol) with gliclazide MR versus sitagliptin
in subgroups according to baseline characteristics
Gliclazide MR vs. sitagliptin
HR (95% CI) Number of participants Number of events P-value for interaction
Sex
Men 1.47 (1.20, 1.79) 1176 391 0.187
Women 1.18 (0.93, 1.52) 810 255
Ethnicity
South-east Asian 1.11 (0.46, 2.67) 62 20 0.656
White European 1.37 (1.05, 1.78) 691 224
Baseline kidney disease
Yes 1.33 (0.92, 1.93) 316 113 0.954
No 1.35 (1.14, 1.60) 1670 533
Baseline CVD a
Yes 1.73 (1.28, 2.34) 558 177 0.056
No 1.23 (1.02, 1.47) 1428 469
Abbreviations: CI, confidence interval; CVD, cardiovascular disease; HR, hazard ratio; MR, modified release.
a Chronic coronary syndromes, cerebrovascular accident, heart failure, peripheral vascular disease, other vascular diseases.
between populations. hd-PS matching of populations from claims or measurements for the baseline covariates used for hd-PS matching.
other databases uses algorithms to select covariates and match HbA1c measurements in patients with controlled glycaemia may be
patients, mitigating selection bias and managing confounding factors, less frequently reported in real-world studies. Furthermore, while we
resulting in real-world treatment groups with similar characteristics. 16 used three HbA1c outcomes to compare the two medications, it
As randomized trials comparing all combinations of individual T2D should be noted that individualized HbA1c targets are increasingly
medications are not feasible, hd-PS matching is a cost-effective tool suggested and used in clinical practices. Background information on
that can be used to examine comparative effectiveness in electronic metformin dose was also not well recorded for most of the included
health record databases. 16 participants; therefore, a proportion of patients may have received
Because of the non-interventional nature and similarly to other lower doses of metformin because of factors such as gastrointestinal
investigations using routinely collected electronic health records, this side effects at the time of prescription of a second-line therapy. Physi-
study has limitations. Data quality of outcomes and other covariates cians may be more likely to prescribe an SU to patients on low-dose
were not standardized across all centres contributing to the CPRD. metformin because of gastrointestinal side effects than other medica-
Thus, there may be variation in data entry or methods used to record tions that might worsen gastrointestinal side effects. Similarly, data