
Page 36 - Rapid Review of ECG Interpretation in Small Animal Practice, 2nd Edition
P. 36
Approach to Evaluating Arrhythmias
VetBooks.ir
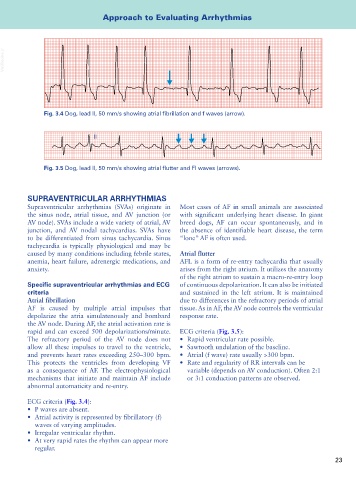
Fig. 3.4 Dog, lead II, 50 mm/s showing atrial fibrillation and f waves (arrow).
II
Fig. 3.5 Dog, lead II, 50 mm/s showing atrial flutter and Fl waves (arrows).
SUPRAVENTRICULAR ARRHYTHMIAS
Supraventricular arrhythmias (SVAs) originate in Most cases of AF in small animals are associated
the sinus node, atrial tissue, and AV junction (or with significant underlying heart disease. In giant
AV node). SVAs include a wide variety of atrial, AV breed dogs, AF can occur spontaneously, and in
junction, and AV nodal tachycardias. SVAs have the absence of identifiable heart disease, the term
to be differentiated from sinus tachycardia. Sinus “lone” AF is often used.
tachycardia is typically physiological and may be
caused by many conditions including febrile states, Atrial flutter
anemia, heart failure, adrenergic medications, and AFL is a form of re-entry tachycardia that usually
anxiety. arises from the right atrium. It utilizes the anatomy
of the right atrium to sustain a macro-re-entry loop
Specific supraventricular arrhythmias and ECG of continuous depolarization. It can also be initiated
criteria and sustained in the left atrium. It is maintained
Atrial fibrillation due to differences in the refractory periods of atrial
AF is caused by multiple atrial impulses that tissue. As in AF, the AV node controls the ventricular
depolarize the atria simulatenously and bombard response rate.
the AV node. During AF, the atrial activation rate is
rapid and can exceed 500 depolarizations/minute. ECG criteria (Fig. 3.5):
The refractory period of the AV node does not • Rapid ventricular rate possible.
allow all these impulses to travel to the ventricle, • Sawtooth undulation of the baseline.
and prevents heart rates exceeding 250–300 bpm. • Atrial (f wave) rate usually >300 bpm.
This protects the ventricles from developing VF • Rate and regularity of RR intervals can be
as a consequence of AF. The electrophysiological variable (depends on AV conduction). Often 2:1
mechanisms that initiate and maintain AF include or 3:1 conduction patterns are observed.
abnormal automaticity and re-entry.
ECG criteria (Fig. 3.4):
• P waves are absent.
• Atrial activity is represented by fibrillatory (f)
waves of varying amplitudes.
• Irregular ventricular rhythm.
• At very rapid rates the rhythm can appear more
regular.
23