
Page 25 - 2021 Medical Plan SPD
P. 25
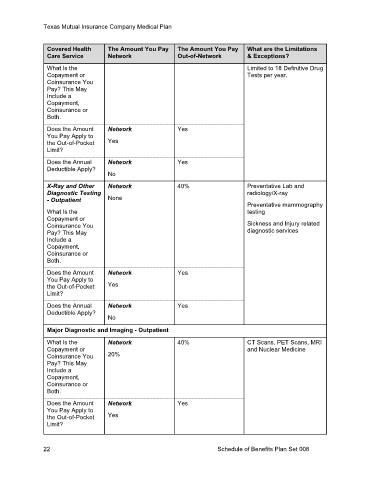
Texas Mutual Insurance Company Medical Plan
Covered Health The Amount You Pay The Amount You Pay What are the Limitations
Care Service Network Out-of-Network & Exceptions?
What Is the Limited to 18 Definitive Drug
Copayment or Tests per year.
Coinsurance You
Pay? This May
Include a
Copayment,
Coinsurance or
Both.
Does the Amount Network Yes
You Pay Apply to
the Out-of-Pocket Yes
Limit?
Does the Annual Network Yes
Deductible Apply?
No
X-Ray and Other Network 40% Preventative Lab and
Diagnostic Testing radiology/X-ray
- Outpatient None Preventative mammography
What Is the testing
Copayment or
Coinsurance You Sickness and Injury related
Pay? This May diagnostic services
Include a
Copayment,
Coinsurance or
Both.
Does the Amount Network Yes
You Pay Apply to
the Out-of-Pocket Yes
Limit?
Does the Annual Network Yes
Deductible Apply?
No
Major Diagnostic and Imaging - Outpatient
What Is the Network 40% CT Scans, PET Scans, MRI
Copayment or and Nuclear Medicine
Coinsurance You 20%
Pay? This May
Include a
Copayment,
Coinsurance or
Both.
Does the Amount Network Yes
You Pay Apply to
the Out-of-Pocket Yes
Limit?
22 Schedule of Benefits Plan Set 008