
Page 28 - 2021 Medical Plan SPD
P. 28
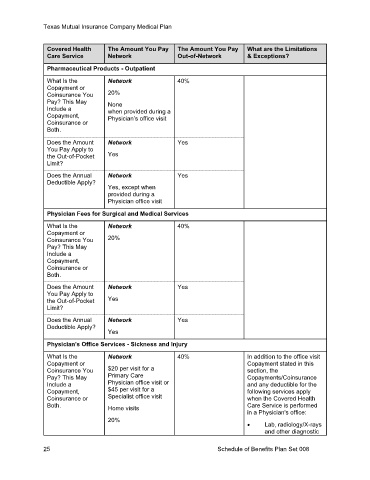
Texas Mutual Insurance Company Medical Plan
Covered Health The Amount You Pay The Amount You Pay What are the Limitations
Care Service Network Out-of-Network & Exceptions?
Pharmaceutical Products - Outpatient
What Is the Network 40%
Copayment or
Coinsurance You 20%
Pay? This May None
Include a when provided during a
Copayment, Physician’s office visit
Coinsurance or
Both.
Does the Amount Network Yes
You Pay Apply to
the Out-of-Pocket Yes
Limit?
Does the Annual Network Yes
Deductible Apply?
Yes, except when
provided during a
Physician office visit
Physician Fees for Surgical and Medical Services
What Is the Network 40%
Copayment or
Coinsurance You 20%
Pay? This May
Include a
Copayment,
Coinsurance or
Both.
Does the Amount Network Yes
You Pay Apply to
the Out-of-Pocket Yes
Limit?
Does the Annual Network Yes
Deductible Apply?
Yes
Physician's Office Services - Sickness and Injury
What Is the Network 40% In addition to the office visit
Copayment or Copayment stated in this
Coinsurance You $20 per visit for a section, the
Pay? This May Primary Care Copayments/Coinsurance
Include a Physician office visit or and any deductible for the
Copayment, $45 per visit for a following services apply
Coinsurance or Specialist office visit when the Covered Health
Both. Home visits Care Service is performed
in a Physician's office:
20%
• Lab, radiology/X-rays
and other diagnostic
25 Schedule of Benefits Plan Set 008