
Page 30 - 2021 Medical Plan SPD
P. 30
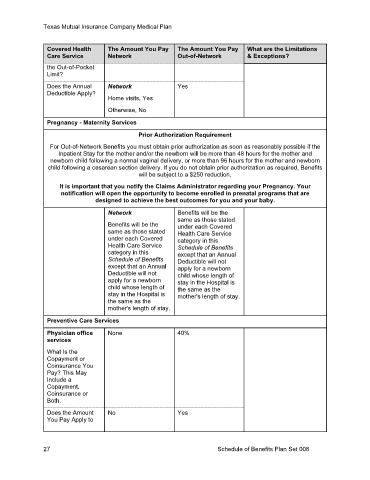
Texas Mutual Insurance Company Medical Plan
Covered Health The Amount You Pay The Amount You Pay What are the Limitations
Care Service Network Out-of-Network & Exceptions?
the Out-of-Pocket
Limit?
Does the Annual Network Yes
Deductible Apply?
Home visits, Yes
Otherwise, No
Pregnancy - Maternity Services
Prior Authorization Requirement
For Out-of-Network Benefits you must obtain prior authorization as soon as reasonably possible if the
Inpatient Stay for the mother and/or the newborn will be more than 48 hours for the mother and
newborn child following a normal vaginal delivery, or more than 96 hours for the mother and newborn
child following a cesarean section delivery. If you do not obtain prior authorization as required, Benefits
will be subject to a $250 reduction.
It is important that you notify the Claims Administrator regarding your Pregnancy. Your
notification will open the opportunity to become enrolled in prenatal programs that are
designed to achieve the best outcomes for you and your baby.
Network Benefits will be the
same as those stated
Benefits will be the under each Covered
same as those stated Health Care Service
under each Covered category in this
Health Care Service Schedule of Benefits
category in this except that an Annual
Schedule of Benefits Deductible will not
except that an Annual apply for a newborn
Deductible will not child whose length of
apply for a newborn stay in the Hospital is
child whose length of the same as the
stay in the Hospital is mother's length of stay.
the same as the
mother's length of stay.
Preventive Care Services
Physician office None 40%
services
What Is the
Copayment or
Coinsurance You
Pay? This May
Include a
Copayment,
Coinsurance or
Both.
Does the Amount No Yes
You Pay Apply to
27 Schedule of Benefits Plan Set 008