
Page 1029 - Small Animal Internal Medicine, 6th Edition
P. 1029
CHAPTER 56 Clinical Conditions of the Dog and Tom 1001
therapy based on sensitivity profiles, keeping in mind pen-
etration into the prostate gland. Appropriate antimicrobial
VetBooks.ir therapy should continue for a minimum of 2 to 8 weeks,
longer in the case of chronic bacterial prostatitis (see later
section). The prognosis for fertility is guarded (but not hope-
less) even with therapy—thermal damage from heat associ-
ated with inflammation impacts spermatogenesis, and the
potential for sperm autoantibody formation exists after such
an inflammatory process; clients should be warned of this
potential complication.
PROSTATIC DISORDERS IN THE
VALUABLE STUD DOG
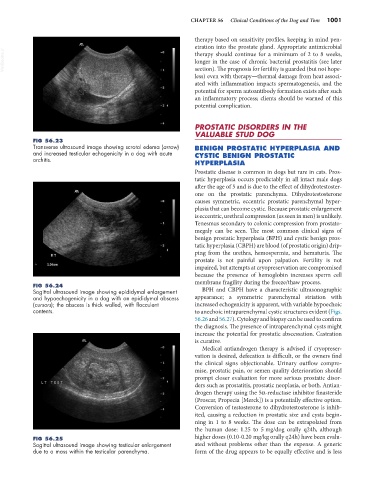
FIG 56.23
Transverse ultrasound image showing scrotal edema (arrow) BENIGN PROSTATIC HYPERPLASIA AND
and increased testicular echogenicity in a dog with acute CYSTIC BENIGN PROSTATIC
orchitis.
HYPERPLASIA
Prostatic disease is common in dogs but rare in cats. Pros-
tatic hyperplasia occurs predictably in all intact male dogs
after the age of 5 and is due to the effect of dihydrotestoster-
one on the prostatic parenchyma. Dihydrotestosterone
causes symmetric, eccentric prostatic parenchymal hyper-
plasia that can become cystic. Because prostatic enlargement
is eccentric, urethral compression (as seen in men) is unlikely.
Tenesmus secondary to colonic compression from prostato-
megaly can be seen. The most common clinical signs of
benign prostatic hyperplasia (BPH) and cystic benign pros-
tatic hyperplasia (CBPH) are blood (of prostatic origin) drip-
ping from the urethra, hemospermia, and hematuria. The
prostate is not painful upon palpation. Fertility is not
impaired, but attempts at cryopreservation are compromised
because the presence of hemoglobin increases sperm cell
membrane fragility during the freeze/thaw process.
FIG 56.24
Sagittal ultrasound image showing epididymal enlargement BPH and CBPH have a characteristic ultrasonographic
and hypoechogenicity in a dog with an epididymal abscess appearance; a symmetric parenchymal striation with
(cursors); the abscess is thick walled, with flocculent increased echogenicity is apparent, with variable hypoechoic
contents. to anechoic intraparenchymal cystic structures evident (Figs.
56.26 and 56.27). Cytology and biopsy can be used to confirm
the diagnosis. The presence of intraparenchymal cysts might
increase the potential for prostatic abscessation. Castration
is curative.
Medical antiandrogen therapy is advised if cryopreser-
vation is desired, defecation is difficult, or the owners find
the clinical signs objectionable. Urinary outflow compro-
mise, prostatic pain, or semen quality deterioration should
prompt closer evaluation for more serious prostatic disor-
ders such as prostatitis, prostatic neoplasia, or both. Antian-
drogen therapy using the 5α-reductase inhibitor finasteride
(Proscar, Propecia [Merck]) is a potentially effective option.
Conversion of testosterone to dihydrotestosterone is inhib-
ited, causing a reduction in prostatic size and cysts begin-
ning in 1 to 8 weeks. The dose can be extrapolated from
the human dose: 1.25 to 5 mg/dog orally q24h, although
FIG 56.25 higher doses (0.10-0.20 mg/kg orally q24h) have been evalu-
Sagittal ultrasound image showing testicular enlargement ated without problems other than the expense. A generic
due to a mass within the testicular parenchyma. form of the drug appears to be equally effective and is less