
Page 816 - Adams and Stashak's Lameness in Horses, 7th Edition
P. 816
782 Chapter 6
ROI values lateroflexion and rotation in the lumbosacral and sacro-
iliac region. The rider should make the horse bend on
VetBooks.ir Right the circles and gradually reduce the circle to a smaller
diameter, thus increasing lateroflexion.
In the fourth month of rehabilitation, the same exercises
Right
are done at the walk and also at the trot to increase speed
and thus loading of the lumbosacral and sacroiliac region.
In the last 2 months of rehabilitation, the horse is
ridden for longer periods, until achieving 1–1.5 hours
of work daily. The canter is introduced with emphasis
on brief episodes with many downward transitions to
trot, creating more dorsal and ventral flexion in the
lumbosacral and sacroiliac region. Short intervals of
canter are extremely important to prevent fatigue of the
muscles that support flexion and extension of the joints
and their supporting ligaments to avoid mobility
beyond their physical limits, which may be diminished
by the primary injury.
10 cm This rehabilitation program gradually introduces
more mobility and develops better muscle support of the
sacroiliac region. The exercises develop more muscle
0cm power in the epaxial muscles as well as in the muscles of
Name Pixel cm 2 cpm cpm/cm 2 the croup, which are of eminent importance in limiting
ROI 1 470 26.7 3174 118 the range of motion of the sacroiliac joints and their
ROI 2 472 26.8 2769 103 supportive ligamentous tissue.
When the sacroiliac joints are involved (in the author’s
Name ROI 1=100% ROI 2=100%
ROI 1 100.00 114.56 practice this is only 10–15% of all cases and is almost
ROI 2 87.29 100.00 always unilateral), injection of the joint with a corticos-
2
Quotient (%): cpm/cm /cpm/cm 2 teroid may be needed. The author prefers triamcinolone
to prednisolone, and it causes less tissue irritation (AP
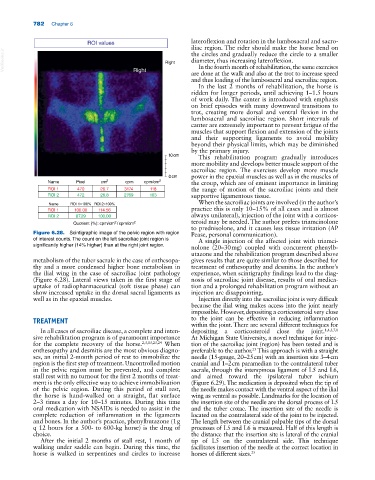
Figure 6.28. Scintigraphic image of the pelvic region with region Pease, personal communication).
of interest counts. The count on the left sacroiliac joint region is A single injection of the affected joint with triamci-
significantly higher (14% higher) than at the right joint region. nolone (20–30 mg) coupled with concurrent phenylb-
utazone and the rehabilitation program described above
metabolism of the tuber sacrale in the case of enthesopa- gives results that are quite similar to those described for
thy and a more condensed higher bone metabolism in treatment of enthesopathy and desmitis. In the author’s
the ilial wing in the case of sacroiliac joint pathology experience, when scintigraphy findings lead to the diag-
(Figure 6.28). Lateral views taken in the first stage of nosis of sacroiliac joint disease, results of oral medica-
uptake of radiopharmaceutical (soft tissue phase) can tion and a prolonged rehabilitation program without an
show increased uptake in the dorsal sacral ligaments as injection are disappointing.
well as in the epaxial muscles. Injection directly into the sacroiliac joint is very difficult
because the ilial wing makes access into the joint nearly
impossible. However, depositing a corticosteroid very close
TREATMENT to the joint can be effective in reducing inflammation
within the joint. There are several different techniques for
In all cases of sacroiliac disease, a complete and inten- depositing a corticosteroid close the joint. 1,4,5,7,8
sive rehabilitation program is of paramount importance At Michigan State University, a novel technique for injec-
for the complete recovery of the horse. 2,3,13,23,24 When tion of the sacroiliac joint (region) has been tested and is
enthesopathy and desmitis are the most obvious diagno- preferable to the author. This approach is with a straight
25
ses, an initial 2‐month period of rest to immobilize the needle (15‐gauge, 20–25 cm) with an insertion site 3–4 cm
region is the first step of treatment. Uncontrolled motion cranial and 1–2 cm paramedian to the contralateral tuber
in the pelvic region must be prevented, and complete sacrale, through the interspinous ligament of L5 and L6,
stall rest with no turnout for the first 2 months of treat- and aimed toward the ipsilateral tuber ischium
ment is the only effective way to achieve immobilization (Figure 6.29). The medication is deposited when the tip of
of the pelvic region. During this period of stall rest, the needle makes contact with the ventral aspect of the ilial
the horse is hand‐walked on a straight, flat surface wing as ventral as possible. Landmarks for the location of
2–3 times a day for 10–15 minutes. During this time the insertion site of the needle are the dorsal process of L5
oral medication with NSAIDs is needed to assist in the and the tuber coxae. The insertion site of the needle is
complete reduction of inflammation in the ligaments located on the contralateral side of the joint to be injected.
and bones. In the author’s practice, phenylbutazone (1 g The length between the cranial palpable tips of the dorsal
q 12 hours for a 500‐ to 600‐kg horse) is the drug of processes of L5 and L6 is measured. Half of this length is
choice. the distance that the insertion site is lateral of the cranial
After the initial 2 months of stall rest, 1 month of tip of L5 on the contralateral side. This technique
walking under saddle can begin. During this time, the facilitates insertion of the needle at the correct location in
horse is walked in serpentines and circles to increase horses of different sizes. 25