
Page 274 - Clinical Small Animal Internal Medicine
P. 274
242 Section 3 Cardiovascular Disease
VetBooks.ir
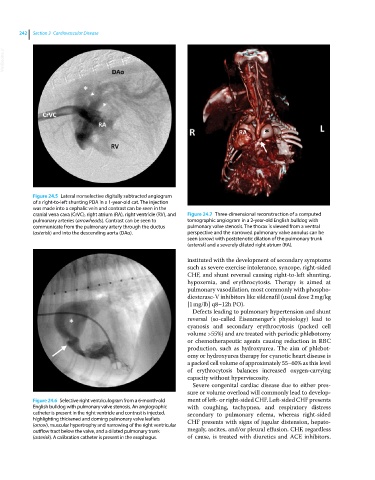
Figure 24.5 Lateral nonselective digitally subtracted angiogram
of a right‐to‐left shunting PDA in a 1‐year‐old cat. The injection
was made into a cephalic vein and contrast can be seen in the
cranial vena cava (CrVC), right atrium (RA), right ventricle (RV), and Figure 24.7 Three‐dimensional reconstruction of a computed
pulmonary arteries (arrowheads). Contrast can be seen to tomographic angiogram in a 2‐year‐old English bulldog with
communicate from the pulmonary artery through the ductus pulmonary valve stenosis. The thorax is viewed from a ventral
(asterisk) and into the descending aorta (DAo). perspective and the narrowed pulmonary valve annulus can be
seen (arrow) with poststenotic dilation of the pulmonary trunk
(asterisk) and a severely dilated right atrium (RA).
instituted with the development of secondary symptoms
such as severe exercise intolerance, syncope, right‐sided
CHF, and shunt reversal causing right‐to‐left shunting,
hypoxemia, and erythrocytosis. Therapy is aimed at
pulmonary vasodilation, most commonly with phospho-
diesterase‐V inhibitors like sildenafil (usual dose 2 mg/kg
[1 mg/lb] q8–12h PO).
Defects leading to pulmonary hypertension and shunt
reversal (so‐called Eisenmenger’s physiology) lead to
cyanosis and secondary erythrocytosis (packed cell
volume >55%) and are treated with periodic phlebotomy
or chemotherapeutic agents causing reduction in RBC
production, such as hydroxyurea. The aim of phlebot-
omy or hydroxyurea therapy for cyanotic heart disease is
a packed cell volume of approximately 55–60% as this level
of erythrocytosis balances increased oxygen‐carrying
capacity without hyperviscosity.
Severe congenital cardiac disease due to either pres-
sure or volume overload will commonly lead to develop-
Figure 24.6 Selective right ventriculogram from a 6‐month‐old ment of left‐ or right‐sided CHF. Left‐sided CHF presents
English bulldog with pulmonary valve stenosis. An angiographic with coughing, tachypnea, and respiratory distress
catheter is present in the right ventricle and contrast is injected, secondary to pulmonary edema, whereas right‐sided
highlighting thickened and doming pulmonary valve leaflets CHF presents with signs of jugular distension, hepato-
(arrow), muscular hypertrophy and narrowing of the right ventricular
outflow tract below the valve, and a dilated pulmonary trunk megaly, ascites, and/or pleural effusion. CHF, regardless
(asterisk). A calibration catheter is present in the esophagus. of cause, is treated with diuretics and ACE inhibitors.