
Page 9 - 2022 Clarins Benefit Guide
P. 9
YOUR BENEFITS GUIDE 2022
Dental and Vision Coverage
Dental Coverage
Regular dental exams can help you and your dentist detect problems in early stages when treatment
is simpler and costs are lower. Keeping your teeth and gums clean and healthy will help prevent most
tooth decay and periodontal disease, and is an important part of maintaining your medical health.
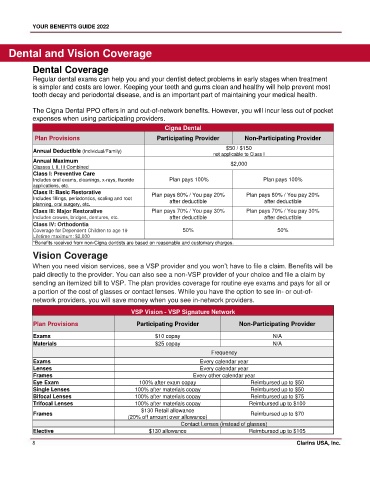
The Cigna Dental PPO offers in and out-of-network benefits. However, you will incur less out of pocket
expenses when using participating providers.
Cigna Dental
Plan Provisions Participating Provider Non-Participating Provider
$50 / $150
Annual Deductible (Individual/Family)
not applicable to Class I
Annual Maximum $2,000
Classes I, II, III Combined
Class I: Preventive Care
Includes oral exams, cleanings, x-rays, fluoride Plan pays 100% Plan pays 100%
applications, etc.
Class II: Basic Restorative Plan pays 80% / You pay 20% Plan pays 80% / You pay 20%
Includes fillings, periodontics, scaling and root after deductible after deductible
planning, oral surgery, etc.
Class III: Major Restorative Plan pays 70% / You pay 30% Plan pays 70% / You pay 30%
Includes crowns, bridges, dentures, etc. after deductible after deductible
Class IV: Orthodontia
Coverage for Dependent Children to age 19 50% 50%
Lifetime maximum: $2,000
*Benefits received from non-Cigna dentists are based on reasonable and customary charges.
Vision Coverage
When you need vision services, see a VSP provider and you won’t have to file a claim. Benefits will be
paid directly to the provider. You can also see a non-VSP provider of your choice and file a claim by
sending an itemized bill to VSP. The plan provides coverage for routine eye exams and pays for all or
a portion of the cost of glasses or contact lenses. While you have the option to see in- or out-of-
network providers, you will save money when you see in-network providers.
VSP Vision - VSP Signature Network
Plan Provisions Participating Provider Non-Participating Provider
Exams $10 copay N/A
Materials $25 copay N/A
Frequency
Exams Every calendar year
Lenses Every calendar year
Frames Every other calendar year
Eye Exam 100% after exam copay Reimbursed up to $50
Single Lenses 100% after materials copay Reimbursed up to $50
Bifocal Lenses 100% after materials copay Reimbursed up to $75
Trifocal Lenses 100% after materials copay Reimbursed up to $100
$130 Retail allowance
Frames Reimbursed up to $70
(20% off amount over allowance)
Contact Lenses (instead of glasses)
Elective $130 allowance Reimbursed up to $105
8 Clarins USA, Inc.