
Page 391 - Feline diagnostic imaging
P. 391
400 23 Liver
(a) (b)
Figure 23.44 Ultrasound images (a,b) of a 15-year-old DSH presented for elevated liver enzymes. Multiple linear hyperechoic
structures are noted within the liver parenchyma. The mineralization is likely associated with the biliary structures within the liver
and can be seen as an incidental finding in older cats. Source: Images courtesy of Dr Merrilee Holland, Auburn University.
Figure 23.45 Longitudinal image of a liver lobe in a cat with
chronic, complete biliary obstruction secondary to pancreatic
carcinoma. The anechoic tubular structure with no Doppler
signal (bd) represents a dilated intrahepatic duct. Color signal
on either side represents normal hepatic vasculature.
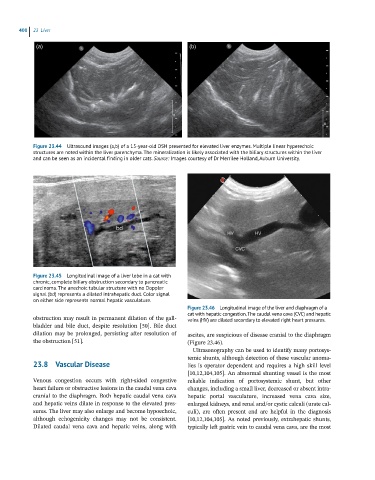
Figure 23.46 Longitudinal image of the liver and diaphragm of a
cat with hepatic congestion. The caudal vena cava (CVC) and hepatic
obstruction may result in permanent dilation of the gall- veins (HV) are dilated secondary to elevated right heart pressures.
bladder and bile duct, despite resolution [50]. Bile duct
dilation may be prolonged, persisting after resolution of ascites, are suspicious of disease cranial to the diaphragm
the obstruction [51]. (Figure 23.46).
Ultrasonography can be used to identify many portosys-
temic shunts, although detection of these vascular anoma-
23.8 Vascular Disease lies is operator dependent and requires a high skill level
[10,12,104,105]. An abnormal shunting vessel is the most
Venous congestion occurs with right‐sided congestive reliable indication of portosystemic shunt, but other
heart failure or obstructive lesions in the caudal vena cava changes, including a small liver, decreased or absent intra-
cranial to the diaphragm. Both hepatic caudal vena cava hepatic portal vasculature, increased vena cava size,
and hepatic veins dilate in response to the elevated pres- enlarged kidneys, and renal and/or cystic calculi (urate cal-
sures. The liver may also enlarge and become hypoechoic, culi), are often present and are helpful in the diagnosis
although echogenicity changes may not be consistent. [10,12,104,105]. As noted previously, extrahepatic shunts,
Dilated caudal vena cava and hepatic veins, along with typically left gastric vein to caudal vena cava, are the most