
Page 404 - Feline diagnostic imaging
P. 404
24.6 Diseisi of tsf eancsei 413
(a) (b)
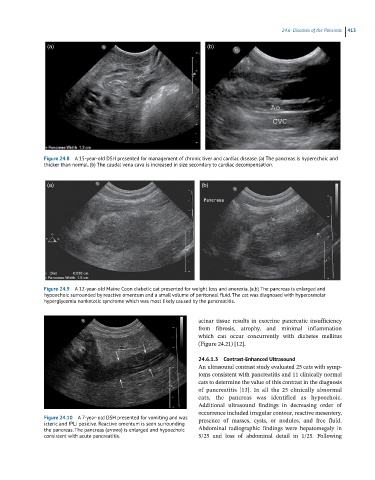
Figure 24.8 A 15-year-old DSH presented for management of chronic liver and cardiac disease. (a) The pancreas is hyperechoic and
thicker than normal. (b) The caudal vena cava is increased in size secondary to cardiac decompensation.
(a) (b)
Figure 24.9 A 12-year-old Maine Coon diabetic cat presented for weight loss and anorexia. (a,b) The pancreas is enlarged and
hypoechoic surrounded by reactive omentum and a small volume of peritoneal fluid. The cat was diagnosed with hyperosmolar
hyperglycemia nonketotic syndrome which was most likely caused by the pancreatitis.
acinar tissue results in exocrine pancreatic insufficiency
from fibrosis, atrophy, and minimal inflammation
which can occur concurrently with diabetes mellitus
(Figure 24.21) [12].
24.6.1.3 Contrast-Enhanced Ultrasound
An ultrasound contrast study evaluated 25 cats with symp-
toms consistent with pancreatitis and 11 clinically normal
cats to determine the value of this contrast in the diagnosis
of pancreatitis [13]. In all the 25 clinically abnormal
cats, the pancreas was identified as hypoechoic.
Additional ultrasound findings in decreasing order of
occurrence included irregular contour, reactive mesentery,
Figure 24.10 A 7-year-old DSH presented for vomiting and was presence of masses, cysts, or nodules, and free fluid.
icteric and fPLI positive. Reactive omentum is seen surrounding
the pancreas. The pancreas (arrows) is enlarged and hypoechoic Abdominal radiographic findings were hepatomegaly in
consistent with acute pancreatitis. 5/25 and loss of abdominal detail in 1/25. Following