
Page 13 - P&A Group Benefits Enrollments Guide
P. 13
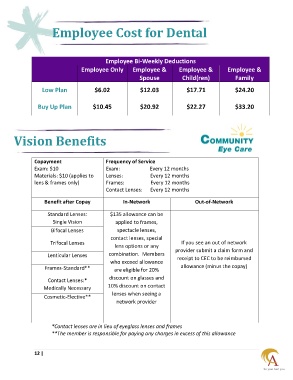
Employee Cost for Dental
Employee Bi-Weekly Deductions
Employee Only Employee & Employee & Employee &
Spouse Child(ren) Family
Low Plan $6.02 $12.03 $17.71 $24.20
Buy Up Plan $10.45 $20.92 $22.27 $33.20
Vision Benefits
Copayment Frequency of Service
Exam: $10 Exam: Every 12 months
Materials: $10 (applies to Lenses: Every 12 months
lens & frames only) Frames: Every 12 months
Contact Lenses: Every 12 months
Benefit after Copay In-Network Out-of-Network
Standard Lenses: $135 allowance can be
Single Vision applied to frames,
Bifocal Lenses spectacle lenses,
contact lenses, special
Trifocal Lenses If you see an out of network
lens options or any
provider submit a claim form and
Lenticular Lenses combination. Members receipt to CEC to be reimbursed
who exceed allowance
Frames-Standard** are eligible for 20% allowance (minus the copay)
discount on glasses and
Contact Lenses:*
10% discount on contact
Medically Necessary
lenses when seeing a
Cosmetic-Elective**
network provider
*Contact lenses are in lieu of eyeglass lenses and frames
**The member is responsible for paying any charges in excess of this allowance
12 |