
Page 503 - Adams and Stashak's Lameness in Horses, 7th Edition
P. 503
Lameness of the Distal Limb 469
In most cases the foot should remain in one of these develop radiographic bone union, but complete osseous
shoes for 6–8 months, with the shoe reset every 4–6 union does not appear to be essential for horses to return
VetBooks.ir restrictive type of shoe (bar shoe only or bar shoe with shod with bar shoes and clips for the remainder of their
weeks. Once clinical improvement has occurred, a less
to athletic activity. In addition horses do not need to be
49
quarter clips) may be used. Horse should not be worked
athletic careers.
44
for approximately 8–10 months, and in some cases, 1 Specific treatment of each type of P3 fracture is given
year of rest may be necessary for clinical improvement. below and included in Table 4.1.
5
Many P3 fractures are very slow to heal and may never
Type I
This nonarticular fracture is best treated with con-
finement and methods to prevent hoof expansion (shoe
or foot cast). However, it may also respond to confinement
and rest alone.
A
Type II
Foals less than 6 months of age should be treated
with stall confinement. Treatment that restricts the
60
expansion of the hoof is usually unnecessary and may
result in severe hoof contraction. Foals should be con-
fined for 6–8 weeks, and their exercise should be
restricted until bony union of the fracture is observed
radiographically. Adult horses can be treated with
confinement and methods to restrict hoof expansion or
surgically by placing a lag screw. However, most type II
fractures are treated nonsurgically because screw place-
47
ment can be very difficult with this fracture type.
Surgery is usually only considered in horses with large
wing fractures.
Type III
This is an unusual fracture in foals and adult horses
B and can be treated similarly to a type II fracture. These
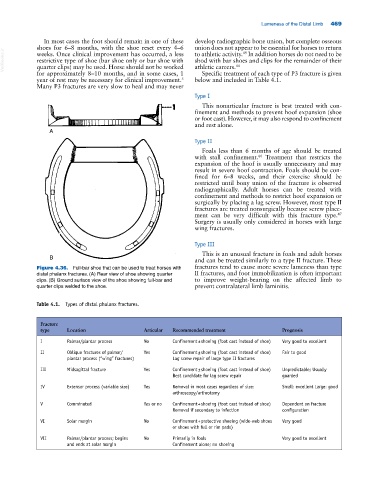
Figure 4.36. Full‐bar shoe that can be used to treat horses with fractures tend to cause more severe lameness than type
distal phalanx fractures. (A) Rear view of shoe showing quarter II fractures, and foot immobilization is often important
clips. (B) Ground surface view of the shoe showing full‐bar and to improve weight‐bearing on the affected limb to
quarter clips welded to the shoe. prevent contralateral limb laminitis.
Table 4.1. Types of distal phalanx fractures.
Fracture
type Location Articular Recommended treatment Prognosis
I Palmar/plantar process No Confinement ± shoeing (foot cast instead of shoe) Very good to excellent
II Oblique fractures of palmar/ Yes Confinement ± shoeing (foot cast instead of shoe) Fair to good
plantar process (“wing” fractures) Lag screw repair of large type II fractures
III Midsagittal fracture Yes Confinement ± shoeing (foot cast instead of shoe) Unpredictable; Usually
Best candidate for lag screw repair guarded
IV Extensor process (variable size) Yes Removal in most cases regardless of size: Small: excellent Large: good
arthroscopy/arthrotomy
V Comminuted Yes or no Confinement + shoeing (foot cast instead of shoe) Dependent on fracture
Removal if secondary to infection configuration
VI Solar margin No Confinement + protective shoeing (wide‐web shoes Very good
or shoes with full or rim pads)
VII Palmar/plantar process; begins No Primarily in foals Very good to excellent
and ends at solar margin Confinement alone; no shoeing