
Page 504 - Adams and Stashak's Lameness in Horses, 7th Edition
P. 504
470 Chapter 4
Acute type III fractures in adult horses are usually the Type IV
best candidates for surgical repair using lag screw fixa- Surgical removal of the fracture/fragment is usually the
VetBooks.ir days duration may fill with granulation/fibrous tissue, preferred treatment for type IV P3 fractures. 9,11,15,38 Acute
Fractures of greater than a few
tion (Figure 4.37).
3,6,24
extensor process fractures are rare in horses and are the
making it difficult to reduce the fracture. However, if
conservative methods are not considered satisfactory, it best candidates for lag screw fixation, but this is rarely
performed (Figure 4.38).
Conservative treatment with
5,36
is feasible to undertake screw fixation several weeks prolonged stall rest is often unsuccessful because the
after the injury, even though the opportunity for inter- extensor process fracture does not heal and horses remain
fragmentary compression is minimized. 25 lame. 15,46 However, most large type IV fractures are
The correct site for screw placement is midway
between the articular surface and solar canal through a chronic, and lag screw repair of these fractures is gener-
ally not recommended. Surgical removal of the extensor
hole in the side of the hoof wall. Screw placement for process fractures/fragments with arthroscopy or a dorsal
24
type III fractures is usually less difficult than for type II arthrotomy is usually the treatment of choice (Figure 4.27).
fractures because the bone is essentially divided in half Arthroscopy using a dorsal approach is the preferred
and there is less risk of splitting the fracture when the technique for removal of small extensor process frac-
screw is tightened. 6,24 The major risks with this proce- tures. 9,11 Large extensor process fractures (greater than
dure are infection developing around the implant, the 1 cm) have also been successfully removed with arthros-
inability to compress the fracture, incorrect screw place- copy by using a motorized burr to help remove the frag-
ment leading to continued lameness, and overriding of ment. 9,15,38 These fractures usually involve a large part of
the fracture fragments during compression. The primary the extensor process (>25% of the joint surface) and can
advantages are less risk of secondary OA developing in be challenging to remove (Figure 4.39). The convales-
9
the DIP joint and faster healing of the fracture due to cence time after removing large fragments is generally
surgical compression. longer than after removing smaller fragments.
Complete fracture healing can be expected in 6–12
months and the screw may have to be removed if lameness
persists or infection around the implant is evident. 3,5,24 A
computer‐assisted surgery (CAS) technique has been
developed to improve accurate screw insertion into sagit-
tal P3 fractures. This technique resulted in greater preci-
2
sion of screw length and placement compared with the
conventional technique and may enable placement of two
screws for improved compression. Improved accuracy of
screw placement can also be accomplished by utilizing CT
24
guidance intraoperatively. Using larger diameter screws
(6.5 or 5.5 mm) has been shown to increase axial com-
pression and reduce the fracture gap of P3 fractures when
compared with 4.5‐mm screws in two separate in vitro
studies. 31,33 Typically, 4.5‐mm screws have been used
because of the small space for screw insertion.
Figure 4.38. A large type IV P3 fracture that may warrant lag
screw repair.
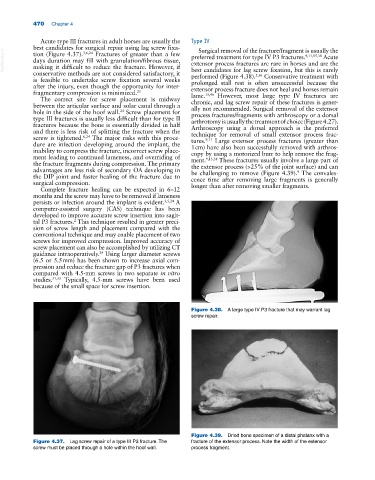
Figure 4.39. Dried bone specimen of a distal phalanx with a
Figure 4.37. Lag screw repair of a type III P3 fracture. The fracture of the extensor process. Note the width of the extensor
screw must be placed through a hole within the hoof wall. process fragment.